A DEXA scan comes back with a T-score below -2.5, the doctor says the word “osteoporosis,” and a marathon goal that felt perfectly reasonable six months ago suddenly feels risky.
Most runners who get that diagnosis hear two conflicting messages from the people around them.
Their doctor says protect the bones and avoid high-impact activity. Their running friends say miles are good for bone density and to keep training.
Neither answer is quite right.
The peer-reviewed research tells a more specific story.
Running alone doesn’t meaningfully rebuild bone density once osteoporosis has set in, and long-distance runners often carry lower bone mineral density than sprinters or power-sport athletes.
Marathon training with osteoporosis can still be a reasonable goal, provided volume, nutrition, and supplemental strength work are built around what the bones actually need.
So, in this article you’re going to learn the research-backed practical advice on marathon training with osteoporosis.
- Whether training for a marathon is safe after an osteoporosis diagnosis
- What running does and doesn’t do to bone density
- How to structure your training week to reduce fracture risk
- The nutrition and strength work that actually move the bone-density needle
- The specific warning signs that mean you need to stop and reassess
Can You Safely Train for a Marathon With Osteoporosis?
For most runners with stable osteoporosis and no history of fragility fractures, supervised marathon training is reasonable.
A 2024 narrative review of masters runners concluded that running at moderate volumes does not appear to cause significant harm to bone health in most athletes, provided energy availability is adequate and strength training is included.

The caveat in that sentence matters.
“Stable” means your bone density has been tracked over at least two DEXA scans, it isn’t rapidly declining, and your doctor has cleared you for high-impact activity.
Runners with a recent fragility fracture, a T-score worse than -3.0, active REDs (low energy availability with menstrual or hormonal disruption), or unmanaged medical conditions that affect bone turnover should stop here and have this conversation with a sports medicine doctor before registering for a marathon.
For everyone else in the osteopenia-to-mild-osteoporosis range, the real question isn’t whether you can run a marathon.
The real question is how to structure the training so the months of impact don’t outpace your bones’ ability to remodel.
The decision is about matching training load to current bone status and building in the strength, fueling, and recovery support the bones need.
What Does Running Actually Do to Your Bones?
Running affects bone in two opposite directions at once.
Impact loading signals bone cells to lay down new tissue, and a 2019 study of club-level marathon runners found that marathoners had higher serum osteocalcin (a bone-formation marker) than age-matched sedentary controls.
That’s the good news.
The less flattering news comes from the wider research base.
A review of bone health in endurance athletes found that distance runners often show lower bone mineral density than athletes in power sports like jumping, sprinting, or team sports, and in some studies lower BMD than sedentary controls.
Two factors explain the gap.
Marathon training rarely produces the peak ground reaction forces that drive the strongest bone-building signal, since easy and steady-state running sits well below the impact threshold associated with meaningful BMD gains.
High training volumes also push runners into low energy availability, which blunts bone formation regardless of the mileage stacked up across the week.
Runners with osteoporosis inherit all of this.
The impact of running doesn’t automatically make bone worse, but it doesn’t reliably make it better either.
Why Long-Distance Running Alone Won’t Rebuild Bone Density
Here’s the part that surprises most runners.
The strongest evidence for rebuilding bone in postmenopausal women with osteoporosis doesn’t come from any aerobic activity, including running.
The LIFTMOR randomized controlled trial showed that 8 months of high-intensity resistance and impact training increased lumbar spine bone mineral density by 2.9% in postmenopausal women with osteopenia or osteoporosis, while the control group lost 1.2% over the same period.
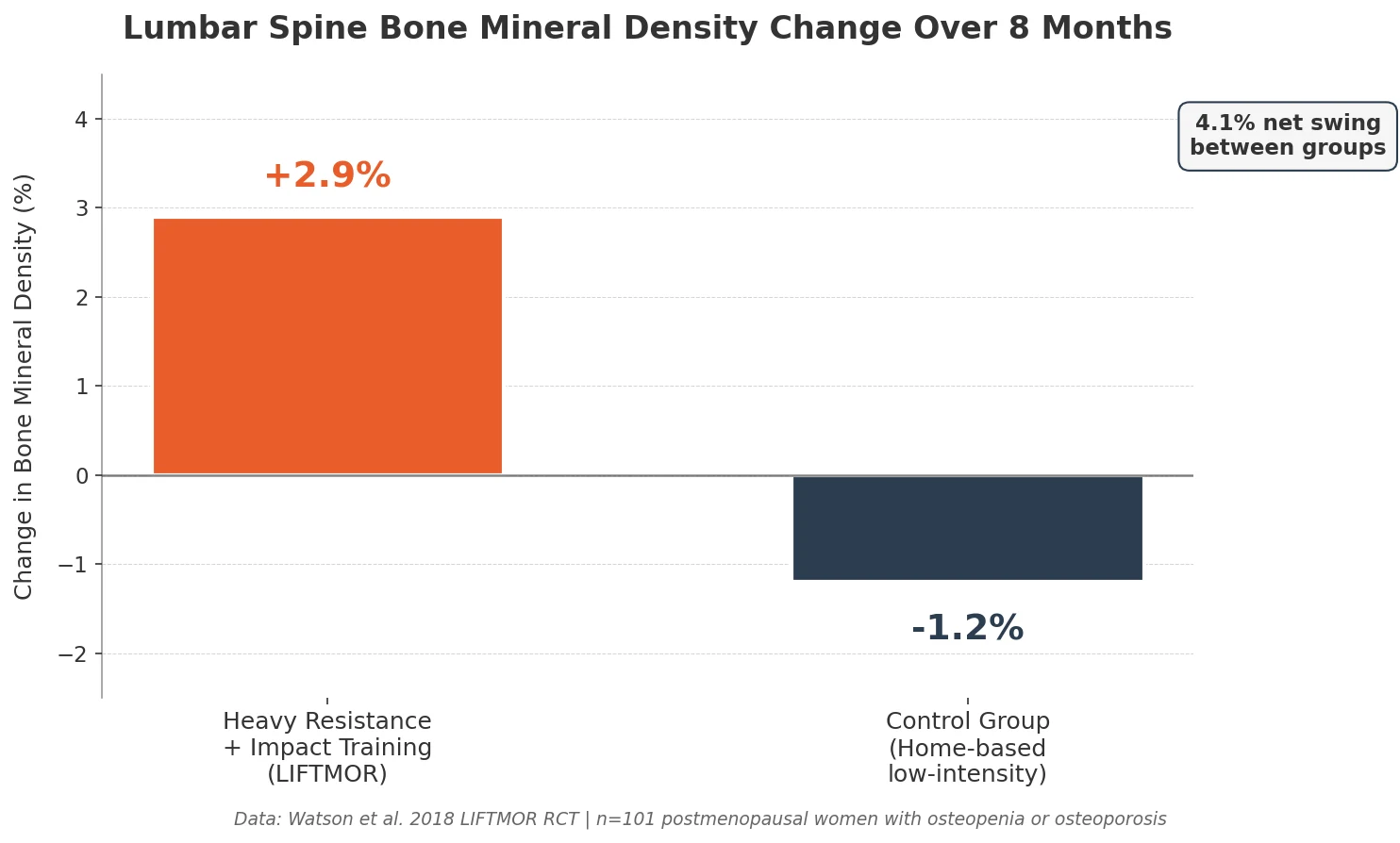
That’s roughly a 4% swing in spine BMD over eight months, in a population where any gain is uncommon.
Femoral neck density and functional strength also improved in the intervention group and declined in the control group.
The intervention wasn’t gentle.
It was heavy deadlifts, overhead press, back squat at loads above 85% of one-rep max, plus jumping drills using a weighted vest, twice a week, supervised.
The LIFTMOR dose isn’t required for every runner with osteoporosis.
The key point is mechanistic: bone adapts to high peak strain, not to accumulated submaximal strain.
A marathon block alone, at training paces in zones 2 and 3, doesn’t supply that peak signal.
Marathon training maintains bones under load, but heavy strength and high-impact work are what actually rebuild bone density.
How to Structure a Bone-Safe Marathon Training Plan
A bone-aware plan looks different from a standard marathon plan in five specific ways.
Run 4 days per week, not 5 or 6.
Every non-running day is a day the skeleton gets to remodel. Dropping from six runs to four, and filling the gap with strength and low-impact cross-training, reduces cumulative bone stress without sacrificing the aerobic adaptations that drive marathon performance.
Cap your weekly mileage at 40 to 45 miles during peak training.
Most sub-4-hour first-time marathoners peak between 35 and 50 miles per week.
Staying on the lower end of that range cuts repetitive loading without compromising race readiness, and longer plans (16 to 20 weeks) allow lower weekly mileage by spreading the build.
Run your easy days on softer surfaces when possible.
Dirt, crushed gravel, and synthetic track surfaces reduce peak ground reaction force compared to concrete. Saving roads for your long run and one workout lets the rest of your week’s miles accumulate on lower-impact terrain.
Do one strength session before easy runs, not after hard sessions.
Heavy lifting on fresh legs produces better mechanical loading and better bone stimulus than lifting under fatigue. Book it the morning of an easy day.
Treat the taper as bone insurance, not just performance prep.
A longer taper (3 weeks instead of 2) and earlier reduction in long-run distance gives your skeleton recovery time that standard plans don’t schedule.
This is also a higher-risk window for stress fracture risk, since runners who feel fresh during taper tend to push pace on easy runs.
| Training Variable | Standard Marathon Plan | Osteoporosis-Adjusted Plan |
|---|---|---|
| Run days per week | 5 to 6 | 4 |
| Peak weekly mileage | 45 to 60 miles | 40 to 45 miles |
| Surface mix | Mostly road | Road for long run and workouts, trail or track for easy |
| Strength work | 1 to 2 sessions, often optional | 2 sessions, heavy load, non-negotiable |
| Taper length | 2 weeks | 3 weeks |
The Nutrition That Protects Your Bones During Marathon Training
Energy availability is the single biggest nutrition lever for bone health during marathon training.
The International Olympic Committee consensus statement on Relative Energy Deficiency in Sport identifies low energy availability as a primary driver of bone loss in endurance athletes, with mechanisms including suppressed estrogen, IGF-1, and thyroid hormones that directly impair bone formation.
Underfueling for even a few weeks during a marathon build pushes the body into a state where it can’t lay down new bone regardless of calcium intake or impact.
Runners with osteoporosis cannot afford any extended period of negative energy balance.
Two targets matter most.
Calcium: 1,200 mg per day
The Institute of Medicine recommends 1,200 mg daily for postmenopausal women and men over 70.
Spread it across the day through dairy, fortified plant milks, leafy greens, and almonds, and supplement only if diet falls short, since excess supplemental calcium may not deliver the same benefit as dietary sources.
Vitamin D: 2,000 IU per day, or titrated to blood level
Vitamin D enables calcium absorption.
A review of stress fracture prevention in young athletes found that calcium and vitamin D supplementation at 2,000 mg calcium and 800 IU vitamin D reduced tibial stress fracture incidence by 20% in female Navy recruits during basic training.
Check 25(OH)D blood levels through your doctor and aim for 30 to 50 ng/mL.
Protein timing matters for bone remodeling.
Protein and calcium balance works together, with adequate protein (1.2 to 1.6 g/kg for endurance athletes in a marathon block) supporting the collagen matrix that calcium mineralizes.
Adequate energy intake is the precondition, and calcium and vitamin D only work if total energy availability is high enough for bone formation to happen.
Why Strength Training Matters More Than Miles for Your Bones
If you add one thing to marathon training after an osteoporosis diagnosis, add heavy strength work.
The LIFTMOR protocol used a specific dose: five sets of five reps at 80 to 85% of one-rep max, on back squat, overhead press, and deadlift, twice per week.
That intensity is what drives the peak bone strain running cannot provide.
You don’t need to replicate the full protocol, but the principle holds.
Progressive heavy loading in compound lifts, done twice a week, carries more bone-building signal than any amount of easy mileage.
Back squat or goblet squat
Loads the hips and spine. Start with bodyweight or a goblet squat, and progress to a loaded barbell squat under a coach’s supervision if possible.
Deadlift
Loads the spine and hips through a hip hinge, which is the same movement pattern that protects your lower back during running. Progress slowly with light dumbbells before going heavier.
Overhead press
Loads the spine axially and recruits the upper body, which distance running largely bypasses.
Hop and jump drills
Brief, multi-directional jumping at the start of a session delivers the high-impact signal bone responds to.
Five sets of 10 hops, landing softly, is a reasonable starting dose for most runners, and you should skip or regress the drill if you have a recent fracture or a spinal compression concern.
Supervised instruction matters more than loading number.
LIFTMOR’s safety record (one minor adverse event across 101 participants) came from trained supervision, so find a strength coach with experience working with osteoporosis before adding loaded barbell work.
RunnersConnect Bonus
Download your FREE Strength Progression slides.
Use these slides to easily create your own progressive strength routine and adapt your strength work to the phase of training you’re in.
When to Pull Back or Stop Marathon Training
Some warning signs mean the current plan has exceeded what your bones can absorb.
Localized bone pain that worsens with activity
Pain that sharpens during a run and lingers afterward, especially in the shin, foot, hip, or pelvis, is the classic stress fracture presentation. Stop running and see a sports medicine doctor within 48 hours.
Pain that shows up at rest or at night
Bone pain that wakes you up or is present when you get out of bed is a red flag distinct from normal training soreness. This requires evaluation before your next run.
A new fragility fracture
Any bone break from a low-impact event (a stumble, a minor fall, a cough) signals bones weaker than your training assumes. Marathon training should pause until your medical team reassesses.
A DEXA showing faster decline than expected
If your bone density drops more than 2 to 3% between annual scans despite the training adjustments, the plan needs rebuilding with your doctor.
Missed or irregular menstrual cycles (for premenopausal women)
Menstrual disruption during marathon training is a symptom of REDs and a direct cause of accelerated bone loss. This is a medical issue that needs addressing before training continues.
None of these signs end running permanently.
They mean the next step is a conversation with your doctor or sports medicine physician, not an internet search.
Marathon training with osteoporosis is viable when the framework stays honest about what the research actually supports.