

Your calf has been tight for months, your knee aches on downhills, and your hip flexors never feel fully loose after a run.
You’ve stretched, foam rolled, and seen your physio twice.
Nothing has stuck.
The source of all three problems might be your big toe.
Hallux limitus is a restriction in the first metatarsophalangeal (MTP) joint, the knuckle where your big toe meets the foot. When that joint can’t move freely during push-off, your body compensates, and those compensations travel up to your calf, knee, and hip.
It’s one of the most under-diagnosed foot conditions in runners precisely because the pain shows up somewhere other than the foot.
In this article, you’ll learn:
- What hallux limitus is and how it differs from hallux rigidus
- Why a restricted big toe shifts load to your ankle, knee, and hip
- A simple standing test you can do right now
- The exercises that restore first MTP mobility
- Which footwear and orthotics changes reduce pain while you train
What Is Hallux Limitus?
Every stride ends with a push-off, and that push-off requires your big toe to bend back toward your shin through the first MTP joint.
Hallux limitus is a restriction in that movement. The joint is limited, not completely locked.
There are two distinct forms, and telling them apart matters for treatment.
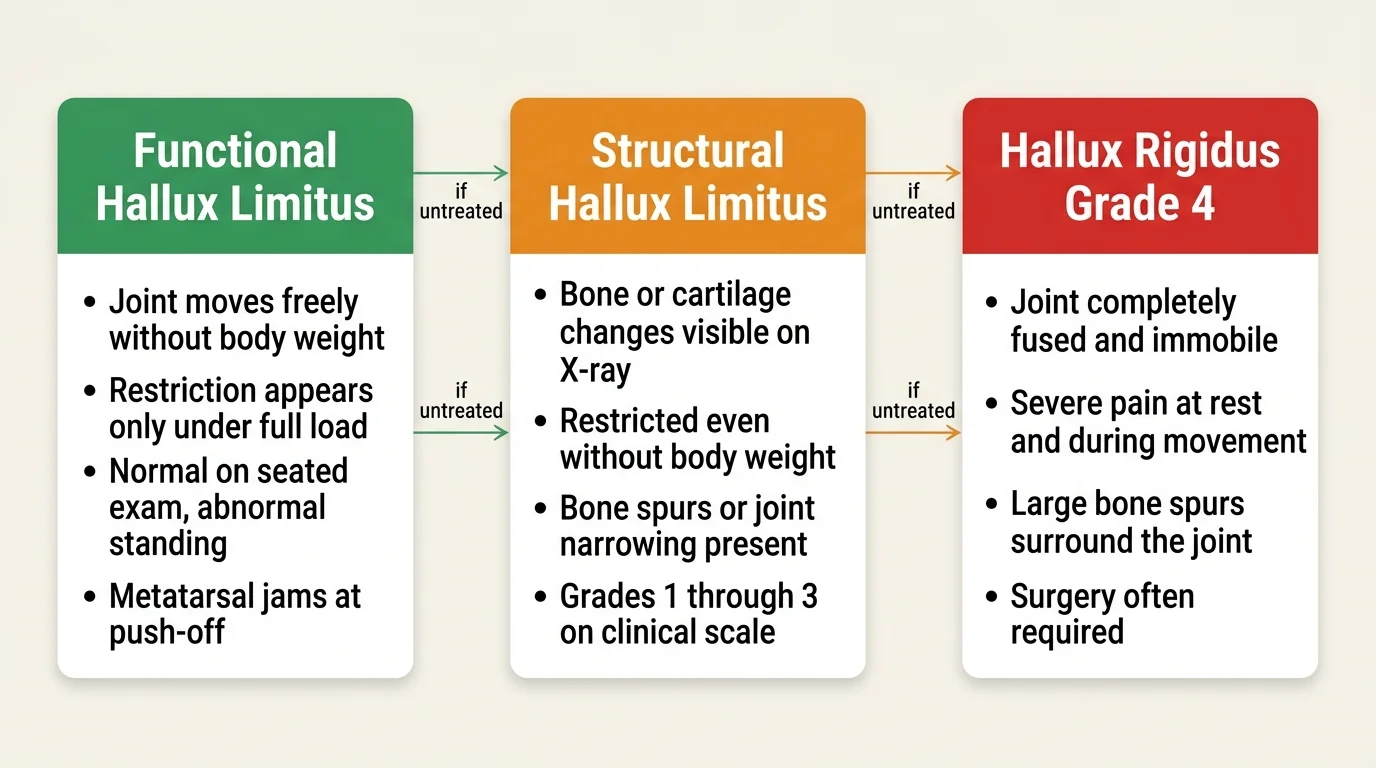
Functional hallux limitus means the joint moves freely when there’s no weight on it but jams under load.
This is the most common form in runners and the easiest to miss, because a standard clinical exam pulling the toe back while seated can look completely normal.
The restriction only appears during the weight-bearing phase of gait, when the metatarsal jams against the base of the toe instead of gliding smoothly.
Functional hallux limitus often goes undiagnosed because the restriction only shows up under load, not during a standard seated clinical exam.
Structural hallux limitus involves actual bone or cartilage changes: arthritis, bone spurs, or joint narrowing visible on X-ray.
Motion is restricted even when non-weight-bearing, and if left untreated, the joint can eventually fuse completely into hallux rigidus.
Clinicians use a Grade 0 to 4 scale to classify severity.
Grade 0 is 40-60 degrees of pain-free dorsiflexion with no symptoms.
Grade 4 is complete fusion with severe degeneration, otherwise known as hallux rigidus.
Most runners presenting with unexplained upstream pain fall somewhere in the Grade 1-2 range.
RunnersConnect Bonus
Download your FREE Injury Assessment and Prediction Video now.
A good injury prevention program starts with assessing where you’re weak and where you might be tight or inhibited. In the video I’ll demonstrate the six mobility tests you need to perform to assess what you need to begin working on.
What Causes Hallux Limitus in Runners?
Normal push-off mechanics depend on a precise coordinated motion between the metatarsal, the big toe, and two small bones underneath the metatarsal head called the sesamoids.
As you approach push-off, the metatarsal needs to plantarflex while the sesamoids slide forward, creating room for the toe to dorsiflex.
When that sliding motion is blocked, the metatarsal jams against the base of the toe on every step.
In runners, the most common causes of that jamming are:
- Overpronation or flat feet: excessive inward foot roll compresses the first ray and blocks normal sesamoid movement
- A tight plantar fascia: the plantar fascia connects to the sesamoid complex, and when stiff it restricts the sliding motion needed for dorsiflexion
- Forefoot-heavy running form: forefoot strikers place repetitive load on the first MTP joint, especially at high mileage
- Narrow or inflexible shoes: shoes that compress the toe box or limit forefoot flex accelerate joint compression
- Previous toe trauma: a stubbed or hyperextended big toe can trigger early-onset functional restriction
A narrow toe box compresses the first MTP joint on every step, making it one of the most underappreciated triggers of hallux limitus in everyday runners.
Repeated jamming also stimulates bone spur growth on the dorsal aspect of the joint.
That bone spur then worsens the mechanical restriction, turning a functional problem into a structural one over time.
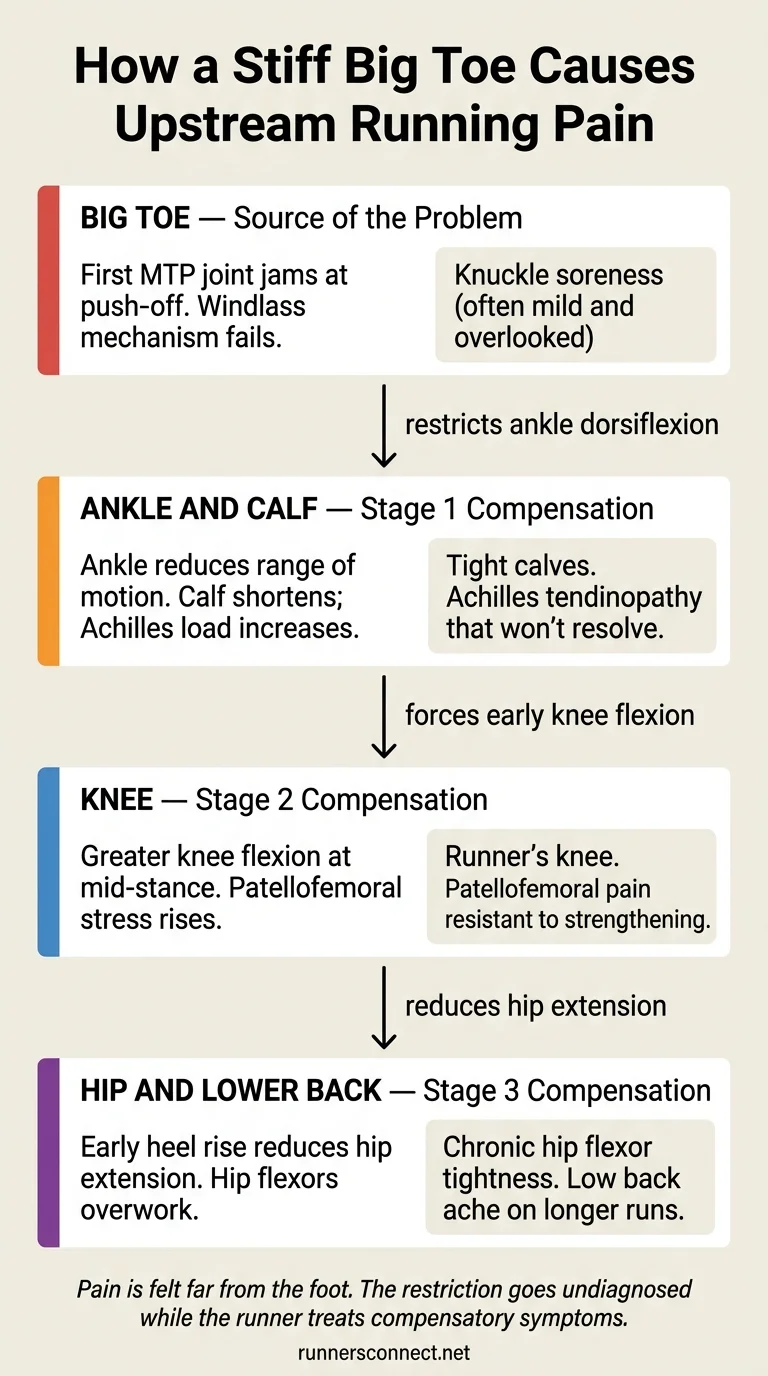
How Does a Stiff Big Toe Cause Ankle, Knee, and Hip Pain?
The reason hallux limitus causes pain far from the foot comes down to the windlass mechanism and basic kinetic chain mechanics.
When the big toe dorsiflexes at push-off, it tensions the plantar fascia, which winds around the arch and stiffens the entire foot for propulsion.
Restrict the toe and that mechanism fails. The foot loses its ability to generate a stable, efficient push-off, and the body has to find another way forward.
Here’s what that compensatory pattern looks like:
Lower leg and Achilles. Limited first MTP dorsiflexion forces the ankle to compensate with reduced dorsiflexion of its own.
The calf never reaches its full stretch in late stance, so it shortens with every stride.
That progressive shortening is why runners with hallux limitus frequently present with tight calves and Achilles tendinopathy that resists standard treatment.
If your calf tightness or Achilles pain doesn’t respond to standard stretching and treatment, a stiff big toe is worth examining before assuming the problem is in the calf itself.
Knee. Reduced ankle dorsiflexion forces earlier and greater knee flexion during the mid-stance phase.
That altered knee mechanics disrupts normal quadriceps loading, increasing patellofemoral joint stress with each stride.
Runners with persistent runner’s knee who don’t respond to hip strengthening or quad work should have their first MTP mobility assessed.
Hip and lower back. The forced early heel rise reduces hip extension in late stance.
The hip flexors have to work harder to compensate for the reduced push-off, which manifests as chronic hip flexor tightness or low back discomfort on longer runs.
How to Tell If You Have Hallux Limitus
There are two tests, and you need both because functional hallux limitus will only show up on one of them.
Non-weight-bearing test. Sit down and use your hand to pull your big toe back toward your shin.
You should get at least 70-90 degrees of passive dorsiflexion without pain.
If this test is restricted, you’re likely dealing with structural hallux limitus involving some degree of bone or cartilage change.
Standing test (Hubscher’s maneuver). Stand on one foot and slowly rise onto your toes.
Watch your big toe: does it bend back smoothly, or does it stiffen and resist as you rise?
Any resistance, rolling to the outer foot, or pain during this test is a positive finding for hallux limitus.
The seated passive test often looks normal in functional hallux limitus, which is why the weight-bearing standing test is the one that actually reveals the restriction.
One detail worth knowing: most runners with hallux limitus experience more pain walking downstairs than running.
Running actually requires slightly less first MTP dorsiflexion range than walking at the same speed, which explains why some runners with mild restriction can complete easy runs but struggle with stairs or hiking downhill.
If self-testing gives consistent positive results, a sports physio or podiatrist can confirm the diagnosis with gait analysis.
An X-ray is needed if you’re in the Grade 3 range with significant joint pain or visible bone enlargement on top of the MTP joint.
What Exercises Help Hallux Limitus?
The most effective conservative approach combines sesamoid mobilization with targeted strengthening of the muscles that stabilize and move the first MTP joint.
Research has shown that participants who received sesamoid mobilization combined with flexor hallucis longus strengthening achieved significantly greater first MTP extension ROM and strength, with significantly lower pain levels after 12 sessions compared to a control group.

These are the three exercises the research supports:
Sesamoid mobilization: sit with your foot flat on the floor and press gently upward on the sesamoid bones, the two small nodules just behind the ball of your foot under the big toe.
Maintain that upward pressure while you dorsiflex the big toe with your other hand.
This mobilizes the sesamoid-metatarsal sliding motion that’s restricted in hallux limitus.
Flexor hallucis longus (FHL) strengthening: place a small towel flat on the floor under your forefoot and scrunch it toward you using only your toes.
The FHL is the muscle that plantarflexes the big toe, and strengthening it improves joint stability and promotes the sesamoid glide that allows dorsiflexion during push-off.
Short-foot exercise: stand barefoot and try to shorten the distance between your heel and the ball of your foot by doming the arch slightly, without curling your toes.
Hold for 5-10 seconds, then release.
The intrinsic foot muscles stabilize the first ray, and weakness in this group is a direct contributor to the jamming mechanics that cause hallux limitus.
| Exercise | Sets x Reps | Frequency |
|---|---|---|
| Sesamoid mobilization | 2 x 10 | Daily |
| Towel scrunches (FHL) | 3 x 15 | Daily |
| Short-foot exercise | 3 x 10-second holds | Daily |
| Single-leg balance | 3 x 30 seconds | 5x per week |
Start with daily frequency and reduce to 5 days per week once joint mobility is improving.
What Footwear and Orthotics Actually Help?
The footwear change that consistently reduces first MTP joint stress in runners is increasing forefoot stiffness.
A shoe that resists flexion at the forefoot reduces how much the big toe needs to dorsiflex during push-off, which decreases the load on an already-restricted joint.
A 2025 study found that a custom anterior forefoot stabiliser orthosis significantly increases first MTP joint stiffness during the propulsion phase, reducing the mechanical demand on a restricted joint during push-off.
Practically, runners with hallux limitus often do better in carbon-plated shoes or any shoe with a rigid forefoot rocker, compared to highly flexible minimalist-style footwear.
For custom orthotics, the most commonly prescribed option is a Morton’s extension: a rigid plate that runs under the big toe and limits dorsiflexion demand at the MTP joint under full body weight.
If you have posterior tibial tendon pain alongside big toe stiffness, a podiatrist-fitted orthotic that also corrects the medial arch will typically outperform an off-the-shelf insert.
You should see a professional if:
- Symptoms have persisted beyond 6-8 weeks despite consistent exercise
- You can see or feel bone enlargement on top of the MTP joint
- Pain is 7 or higher at rest or prevents completion of easy runs
- The non-weight-bearing passive test shows significant restriction
Surgery is rarely required for Grade 1-2 hallux limitus, and most runners with functional or early structural restriction return to full training with consistent exercise and footwear modifications.



20 Responses
Great piece Matt. The importance of the big toe (all toes for that matter) and its role in good foot & ankle range of motion and strength, is too often under appreciated.
Glad you enjoyed it Matt. Thanks for sharing your feedback, we could not agree more!
Hi there. Thanks for the great article. Been struggling with severe pain in my toe- doctor said it’s just a strain and prescribed an anti-inflammatory gel. However, after reading this article and doing the maths, I’m pretty sure that my shoes are the problem as the pain started a couple months after I bought them (that, and that I’ve started developing a bunion on this same toe) Knowing this, is it still necessary that I see a specialist? Also, how long and how much rest is necessary? I’ve just gotten into a good rhyme and am loath to lose my momentum. Any advice is welcomed gratefully. Thanks 🙂
Hi sherrie, thanks for reaching out. Glad you found the article helpful. It would be difficult for us to tell you exactly how much rest to take, as that will be a question for your doctor. We have this article on running shoes, which may be of help to you if you think it is your shoes causing the problem https://runnersconnect.net/running-injury-prevention/how-to-find-the-right-running-shoe/ Best of luck, keep us posted on it!
Hi Sherrie, good to hear the article got you thinking! If you only started struggling with the pain after buying the new shoes, it is definitely worth returning to your old shoes for a while to see if the problem reduces. Watch out for any coinciding rapid changes in your running frequency, intensity or duration as well though as we often subconsciously push our bodies harder after buying new shoes. As for rest, remember that total rest is rarely the answer. You need to be doing suitable mobility and strengthening exercises to help reduce pain and restore function. A sports therapist should be able to help you create a suitable exercise routine once they have assessed you. Thanks again for the comment. Let us know how it goes!
Thanks for the info. My podiatrist just diagnosed hallux limitus for me. The xrays show bone spurs on the top of the metatarsal joint that are causing a jamming of the joint. The strange thing is that i have no pain on the top of my foot. The discomfort is all on the bottom like i have a rock in the middle of my shoe. Turned out to be the swelling is on the bottom caused by the trauma at the top. Just the beginning of the experience for me. Hopefully I have a lot of running left to experience.
Hi Brian, thanks for reaching out and sharing your story. It is good to know that you have a diagnosis for your problem. Now you can begin to work on it, and hopefully the suggestions in this post can help you recover quicker!
Thanks for sharing Brian. Glad the article was of use to you. With the right care, I hope we hear you are happily running again as soon as possible!
I’ve been running with a custom orthotic for hallux limitus for over a year now and going strong!
i am suffering from this hallux limitus..its been 8 months i cant lift my big toe ( of my left leg)..last december i had a tibia plateau fracture..it caused me the nerve injury..is there any exercise i can do for my toe? will it recover..plz let me know
Hi Ieffa, thanks for reaching out. Sorry to hear about your toe. This would be a question for your doctor, as we cannot diagnose you from here, but the suggestions we made in the post should help you recover, and ease off the stress on your toe. Hope this helps!
Hi,
Have been told I have functional hallucinations limitus and was given orthotics. Wore them for several months but my body just couldn’t get used to them. Is surgery an option for functional hallux limitus?
Hello, thanks for reaching out.We did talk about surgery as an option in the post itself, we also suggested alternative options to try to avoid it. Give our suggestions a try and see how you get on!
Hi…I have seen a podiatrist several times. She doesn’t seem very interested in helping with my problem. I am an RN. I believe that I have hallux limitus/rigidus. I have a huge bump on the top of my left big toe (the affected toe) as well. My right big toe is following suit as well. I saw my x-rays. I have had casts made of both feet. And an orthotic set made to wear, several years ago. I tried to wear it. I could only wear it several hours inside the house. It hurt! My pain, Like Brian, is in the ball of my foot. The first indication of a problem was pain in my big toe. And the large bump on the top of my toe. But that is gone now. The Podiatrist says that I have no joint left in my (L) big toe. She gave me topical med to apply to foot. And suggested a New Balance orthotic to try. I also have scoliosis that was fixed with surgery and a Harrington rod when I was 17. But my curvature is back and about the same as before surgery. I need some insight from someone on how to deal with these multiple problems. I realize that my foot is making the rest of my problems worse. But no other Dr. seems to want to do any further evaluation. I need a recommendation for someone in my area (or not. I’m willing to go to them) for a total body evaluation. I obviously do not run. But those who do seem to be getting the best answers and solutions to similar problems. Can you tell me who I might consult? A gait analyst, sports med expert, or someone else? I am tired of trying to find help alone. Regular MD’s don’t seem to be interested in anything except surgeries and meds. Thanks for your time.
Hi Jennifer, I am sorry but we are unable to make suggestions as we do not have access to specialists in particular areas. Sorry to hear about it, but it would be best to look into getting a full body gait analysis, like we talked about in this podcast episode https://runnersconnect.net/rc43 or http://podcast.runnersconnect.net/e/small-changes-that-will-make-a-big-difference-to-your-performance-max-prokopy/
Hope this helps! Sorry we cannot help more!
Great article. It’s extremely important for people to be aware of this early and to make the necessary changes.
I’m 26 years old with severe hallux rigidus that began when I was 19. I’ve had two cheilectomies on my left foot and a first mtp joint osteotomy on my right, and need another operation on each foot in the near future due to the re-degradation of the joints since the most recent operations three years ago.
Every line in this article hits home, as since my toes have degraded steeply once again over the past months, my knee tendinitis has become aggravated again, my calves are constantly as tight as anything, my glutes are strained almost weekly, and my hips/lower back ache.
Over the past two months I’ve gotten three separate opinions, all agreeing that imminent surgery is necessary but disagreeing on the type. I had all but ruled out arthrodesis, but then I saw an orthopedic surgeon yesterday who said the only surgery he would perform in my case would be arthrodesis on both feet. I’m extremely hesitant to permanently fuse the bones at only 26 years old. Have any of you come across runners who have had the arthrodesis performed and still could be active and comfortable? The doctor I saw yesterday assured me people can still do as much as run marathons after the arthrodesis, but I find it hard to believe it’d be comfortable to have two fused big toes for (hopefully) the next 60+ years.
The other option I am considering is arthroplasty, getting joint implants in both feet. Have any of you come across anyone (runner or not) who have had this performed?
Thanks in advance for your time. Been a daily issue in my life for seven years now and like I mentioned, this article hit home more than any other I’ve read on the topic.
Happy to help Mike. Sorry to hear it has been so much trouble for you. We have not got any information about arthroplasty, but if you wish to try it, then we would love to hear your thoughts, you might provide comfort to other runners, and you know how much that would help you to learn what others found help. Thank you for sharing. Best of luck with your recovery!
Hey Guys
Uh, you guys nailed it. My last two seasons I’ve developed a bunion on my right foot limiting my range on that toe. It is manifesting the pain on my left calf due to a poor toe off on my right side. My left calf has taken the brunt of my poor right foot toe off. My coaches are playing with different orthotics and it immediately takes the load off my calf. Any other suggestions? I can’t seem to get it just right as my pain in my calf can move due to alterations in my orthotics.
Thanks….Very good article!
I have this from ballet. Does anyone recommend a pair of sneakers? My 1st metatarsals are fused and I am in pain all the time.
Great article..great mystery injury to identify…feet control so much.
Are there recomended range of motion and strength recomendations? Rolling the towel with our feet for instance?
M