

Your shin starts burning at exactly the same point in every run.
Mile two, sometimes mile three.
The pain is deep inside the muscle, not on the bone.
It fades completely within 20 minutes of stopping.
That pattern is the hallmark of chronic exertional compartment syndrome, a condition that looks like shin splints from the outside but works differently underneath.
Diagnosis takes months on average because the pain vanishes by the time you reach the doctor’s office, and most clinicians don’t measure compartment pressure unless prompted.
In this article, you’ll learn:
- How compartment syndrome differs from shin splints based on location, timing, and bilateral patterns
- What triggers the pressure buildup in runners and who faces the highest risk
- How doctors confirm the diagnosis using a pressure test after exercise
- Whether surgery is necessary, and what a 2012 study suggests about a non-surgical alternative
- How quickly you can return to running after treatment
Is It Compartment Syndrome or Shin Splints?
Both injuries produce lower-leg pain that worsens with running and both are common in distance runners.
The critical distinction is anatomical: shin splints (medial tibial stress syndrome) cause pain directly on the shin bone, while compartment syndrome causes pain inside the muscle belly several centimeters away from the tibia.
If your pain sits directly on the ridge of the shin bone rather than deep in the muscle tissue several centimeters away from the bone, shin splints or a stress fracture is more likely than compartment syndrome.
Timing is the second differentiator.
Shin splints often hurt from the first step, and soreness can persist for hours after a run.
Compartment syndrome has a reliable onset window: you’re pain-free for the first mile or two, pain builds steadily until you stop, and then it clears within 30 minutes of finishing.
A third clue: compartment syndrome affects both legs simultaneously in 60 to 80 percent of cases.
Bilateral muscle pain that appears at the same distance each run, deep in the muscle, with rapid post-run resolution is the classic compartment syndrome profile.
What Causes Compartment Syndrome in Runners?
The muscles of your lower leg sit inside four tight sheaths of connective tissue called fascial compartments.
When you run, blood flow to working muscles increases and they swell by as much as 20 percent in volume.
In most runners, the compartment is large enough to accommodate this expansion without issue.
In runners with chronic exertional compartment syndrome, the fascial sheath is too rigid relative to muscle volume.
Pressure inside the compartment rises sharply during exercise, compressing blood vessels and nerves and producing pain that forces you to slow or stop.
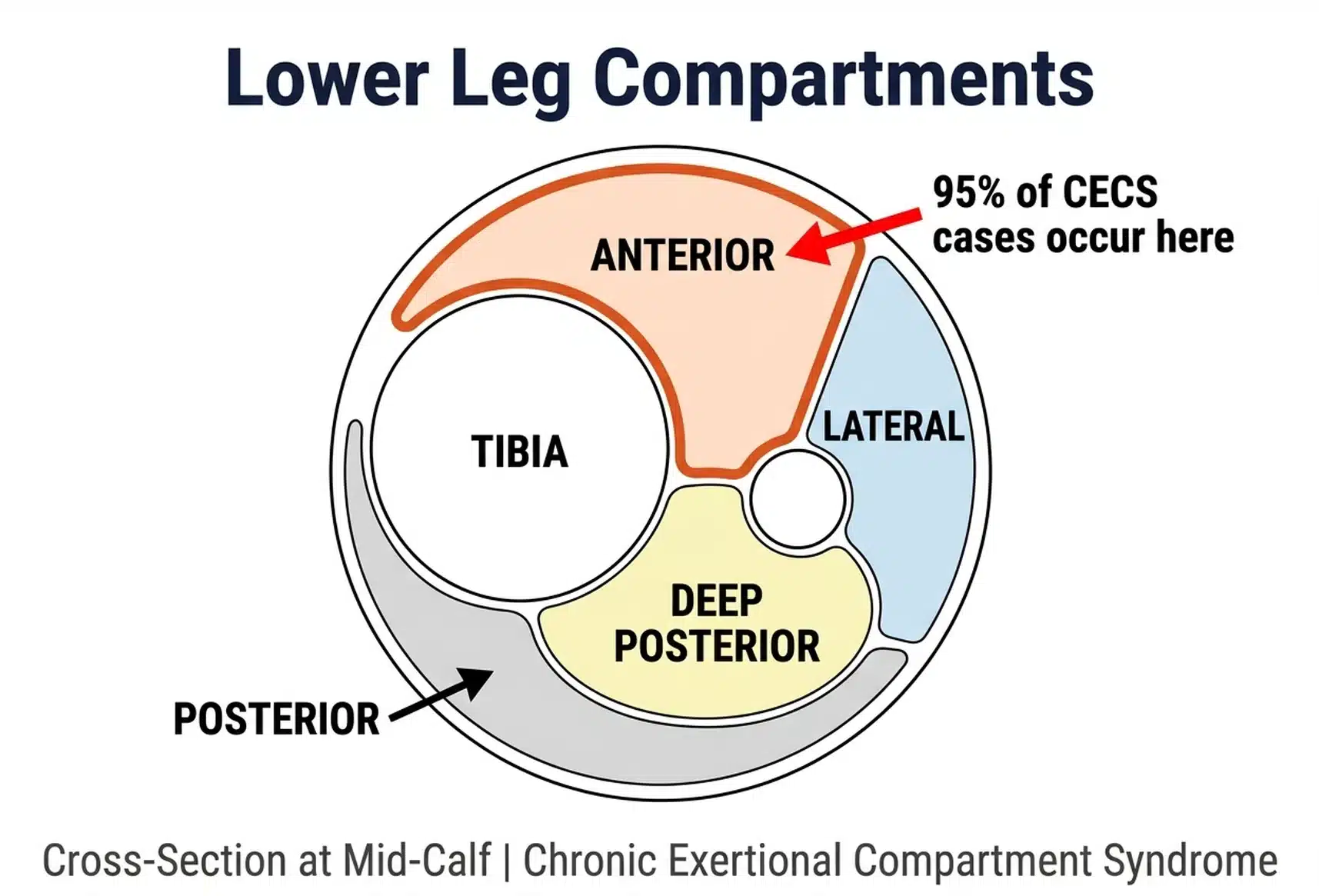
Research has found that 95 percent of chronic exertional compartment syndrome cases occur in the anterior or lateral compartments of the lower leg — the front and outer shin.

This concentration in the anterior compartment matters for treatment: the surgical approach and even the non-surgical options differ based on which compartment is affected.
Compartment syndrome is more common in younger runners.
The median age at symptom onset is around 20 years, which makes sense anatomically: the size of your fascial compartments is fixed once growth stops, and problems tend to emerge when training volume climbs post-adolescence.
Men and women develop it at roughly equal rates.
Some evidence links rearfoot striking and overstriding to higher loading of the anterior compartment, though this is based on biomechanical data rather than prospective injury tracking.
What Are the Symptoms of Compartment Syndrome?
The location of your symptoms depends on which compartment is involved.
Anterior compartment syndrome produces aching, tightness, and burning across the front and slightly outer face of the lower leg, the fleshy area just to the outside of the shin bone.
Posterior compartment syndrome, which is rarer, produces similar symptoms in the calf and back of the lower leg.
Across all types, the hallmark features are:
- Pain that starts after a predictable distance or duration, often the same point every run
- Progressive worsening that forces you to slow or stop
- Complete or near-complete resolution within 15 to 30 minutes of stopping
- Tightness, numbness, or tingling in the foot or lower leg during exercise
- Weakness when trying to pull your toes upward (anterior) or push through a calf raise (posterior)
Pain that disappears within minutes of stopping and returns at the same point in every run is the most reliable single symptom of compartment syndrome, and the feature that most clearly separates it from shin splints or a tibial stress fracture.
In some cases, you’ll feel firm, swollen lumps along the muscle belly during or immediately after a run as the muscle presses against the restricted fascia.
How Do Doctors Diagnose Compartment Syndrome?
Diagnosing compartment syndrome in a clinic is notoriously difficult because the pain disappears quickly once exercise stops.
An MRI or bone scan can rule out tibial stress syndrome and stress fractures, both of which show up clearly on imaging, but neither confirms compartment syndrome.
The gold-standard test is a compartment pressure measurement performed immediately after exercise.
The protocol: you run on a treadmill until you reproduce your symptoms, then a physician inserts a needle-tipped pressure gauge into the affected compartment and records readings within one to five minutes of stopping.
Pressure above established thresholds at the one- and five-minute marks confirms the diagnosis.
Correct diagnosis takes several months on average because pain resolves before most appointments. If you have classic compartment syndrome symptoms and your doctor labels it shin splints without a pressure test, ask specifically about chronic exertional compartment syndrome and request a referral for exercise-based pressure measurement.
The pressure test is mildly uncomfortable but brief, and it closes the diagnostic question definitively.
Does Surgery for Compartment Syndrome Actually Work?
For runners who want to continue training at previous levels, fasciotomy has the strongest evidence of any available treatment.
The procedure involves making small incisions to release the fascial sheath of the affected compartment, creating permanent room for the muscle to expand during exercise.
Studies report that anterior compartment fasciotomy allows 60 to 80 percent of runners to return to their previous level of training, with lower success rates for deep posterior compartment releases.
In roughly 10 percent of cases, symptoms return within months because the initial fascial release was insufficient.
A second procedure is typically needed when recurrence happens.
Recovery timelines are faster than most serious running injuries: incisions heal within one to two weeks, pool running and cycling can begin immediately after, and most runners are back on roads at six to eight weeks post-surgery.
RunnersConnect Bonus
Download our Top 5 exercises to prevent anterior tibialis.
It’s a PDF with images and descriptions of the 5 most effective prevention and rehab exercises for runners with anterior tib issues.
Can You Treat Compartment Syndrome Without Surgery?
Rest, anti-inflammatories, and foam rolling provide temporary relief but don’t resolve the pressure problem once you return to full training volume.
One promising non-surgical alternative is a gait change.
A 2012 study from researchers at West Point tested whether transitioning to a forefoot strike could reduce anterior compartment pressure enough to eliminate symptoms.
Researchers found that ten runners with anterior compartment syndrome who transitioned to forefoot striking over six weeks reduced post-run compartment pressure by more than half, with pain improvements maintained at a one-year follow-up.
The mechanism is mechanical: heel-strike followed by foot slap places peak load on the anterior shin muscles at every footfall.
A forefoot or midfoot strike distributes that load differently, reducing peak pressure in the anterior compartment during the loading phase.
Three caveats matter before you try this:
- Evidence is limited. This was a single study with ten participants and no control group. The results are promising but not yet definitive.
- Compartment specificity. This approach only applies to anterior compartment syndrome. For posterior compartment syndrome, forefoot striking increases loading there and would worsen symptoms.
- Transition injury risk. Rushing a foot-strike change raises the risk of calf strain, Achilles tendinopathy, and metatarsal stress fracture. A six- to eight-week transition with professional guidance is essential.
If you want to try this route before surgery, work with a physio or running coach to guide the transition, then retest compartment pressure after six weeks of consistent forefoot running to see whether the intervention has reduced pressure to normal levels.
How Do You Train and Return to Running After Compartment Syndrome?
Aqua jogging is the most effective cross-training tool during compartment syndrome recovery because it replicates running mechanics in a zero-impact environment.
Research shows that runners who train exclusively with deep water running for four to six weeks maintain aerobic fitness and lactate threshold with no measurable decline in race performance when they return to land.
Stationary cycling works as a secondary option if pool access is limited, though it develops different muscle activation patterns and doesn’t maintain running economy as effectively.
Start aqua jogging immediately, whether you’re waiting for a surgical date, recovering post-surgery, or trialing the forefoot strike approach. There is no benefit to complete rest when a fitness-preserving alternative is available.
Return-to-running timelines depend on the treatment route:
- Post-fasciotomy: Pool running or cycling once incisions heal (week one to two); gradual return to road running starting at week six to eight; full training load by weeks ten to twelve
- Forefoot strike transition: Variable. Outcome depends on how pressure normalizes and how your legs adapt; retesting compartment pressure after six weeks of consistent forefoot running gives you a concrete answer on whether to continue or pursue surgery
Three months from surgery to full mileage is a realistic and common outcome for anterior compartment syndrome, which is a faster timeline than recovery from a tibial stress fracture or a significant tendon injury.


