

We recently posted an article about the research studies behind NuNee and how it’s 90% effective at treating runner’s knee.
In that article, I outlined the literature and results of the specific studies that demonstrated the effectiveness of the NuNee device, but I didn’t dig deep into the why or the how.
So, I thought this would be a good time to talk about the mechanics behind how and why NuNee works with the intent of opening up a broader discussion about running mechanics and specifically how the knee and patella in regards to running mechanics.
What causes runner’s knee
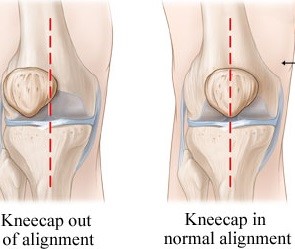
For healthy runners the kneecap, or patella, slides up and down a groove in the end of the femur when you straighten and bend your knee.
However, for runners who suffer from runner’s knee, the patella isn’t able to track properly in this groove.
Thus, the patella rubs up against the edges of this groove in the femur and causes the pain you feel with runner’s knee. Hence the technical term for the injury, “patellofemoral pain syndrome.”
Researchers and biomechanics experts have identified a number of potential underlying causes for why the patella doesn’t track properly. These include muscular weakness or strength imbalances and poor movement coordination.
Regardless of the underlying reason, the result is an abnormal alignment or mal-tracking of the patella.
For example, research has demonstrated that a lack of hip strength or hip muscle coordination can cause the femur to internally rotate knee or “collapse” too much, which misaligns the tracking of the patella.
Other studies have shown that quad strength imbalances can alter the tracking of the kneecap, usually because the imbalance causes one side to “pull” a little too much.
Why traditional braces don’t work
It seems the obvious solution to runner’s knee would then be to wear a brace that either supports the quadriceps to reduce potential imbalances or help realign the femur to prevent internal rotation.
However, there have been several studies conducted on the effectiveness of different braces on treating runner’s knee that have demonstrated some relief in pain, but not an improvement in underlying cause or a significant enough reduction to reduce normal training.
For example, a study examining the immediate effects of an elastic brace on quadriceps muscle activation reported a pain reduction of 33-56 percent, but there was no difference in muscle activation (Kölle et al., 2020).
Another study by McCrory et al., 2007 used a brace which reduced knee extension to treat runner’s knee. While the pain was reduced, no differences were found in lower extremity alignment associated with runner’s knee.
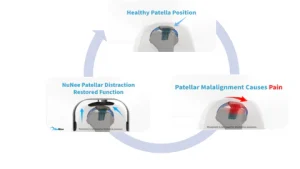
A new approach – Patellar Joint Distraction
Joint distraction is a process that slightly separates the patella from the femur.
It works by applying a “controlled distraction force” across the joint between the femur and patella, which helps relieve the pressure and also helps the patella stabilize to properly align and track to prevent the rubbing against the femur.
In addition to relieving pain, joint distraction can also help to repair and restore cartilage. When the joint is unloaded, the cartilage can absorb more nutrients and oxygen, which can help to promote healing and restore the health of the joint.
Initially, it was only provided as non-invasive surgery, but recent research has shown that the same benefits can be seen when using a brace to apply the joint distraction.
This is how the NuNee device is designed to work. Rather than using traditional bracing techniques, NuNee utilizes the concept of patella joint distraction to relieve pressure on the knee cap.
This is why the literature has shown it eliminates pain in 90% of patients as soon as they put it on.
Recapping the literature
In case you missed our original article, two research studies conducted in 2022 at Nazareth College School of Physical Therapy in Rochester, NY have demonstrated NuNee to be 90% effective at providing both immediate and long-term relief.
Immediate effects
Participants were screened for anterior knee pain using a standardized musculoskeletal exam to rule out causes of knee pain that would exclude participation. They were then asked to identify their current level of pain on a 0-10 numerical rating scale.
Subjects completed a single functional test including stair ambulation, squat or running, depending on what was most provocative.
They completed testing without any type of brace then with the NuNee device, and a pain rating was recorded during each test scenario to identify immediate response.
When engaging in provocative activity, 89% reported decreased pain immediately after donning the NuNee brace.
Results show a mean score of 3.38 on the numerical rating scale with provocative activity without the brace, and 1.62 with the brace, resulting in significant decreases in reported pain. Five participants also reported improvements in their pain at rest when wearing the brace.
6 week follow-up
After six weeks, participants demonstrated statistically and clinically significant changes in Kujala and numerical rating scale scores. The Kujala test is a 13-item screening instrument designed to assess patellofemoral pain in adolescents and young adults.
During functional testing at follow up, 100% of participants reported pain scores of 0/10 while using the brace.
These findings suggest that the NuNee brace can reduce immediate and long-term pain and improve function when worn during physical activity in individuals with anterior knee pain.
If you are suffering from runner’s knee and want to give NuNee a try, head to nuneeshop.com. They offer a 100% moneyback guarantee if it doesn’t work for you, so there’s no risk to give a it a try.



