

Pain along the front of your ankle or the bottom of your shin is one of those signals most runners try to push through, assuming it’ll resolve on its own.
If that pain tracks along a thin line from your lower shin, cuts diagonally across the front of the ankle, and settles near the top of your foot, the tibialis anterior tendon is almost certainly involved.
Anterior tibialis tendonitis, also called tibialis anterior tendinopathy, is one of the less common running injuries, which makes accurate information genuinely hard to find.
So, in this article you’re going to learn the research-backed practical advice on:
- What the tibialis anterior does during your running stride and why it’s vulnerable at heelstrike
- How to tell anterior tibialis tendonitis apart from a stress fracture or compartment syndrome before you see a doctor
- The specific footwear adjustments and exercises that reduce strain and speed recovery
- The pain monitoring rule that tells you whether you can keep running or need to rest
What Does the Tibialis Anterior Do When You Run?
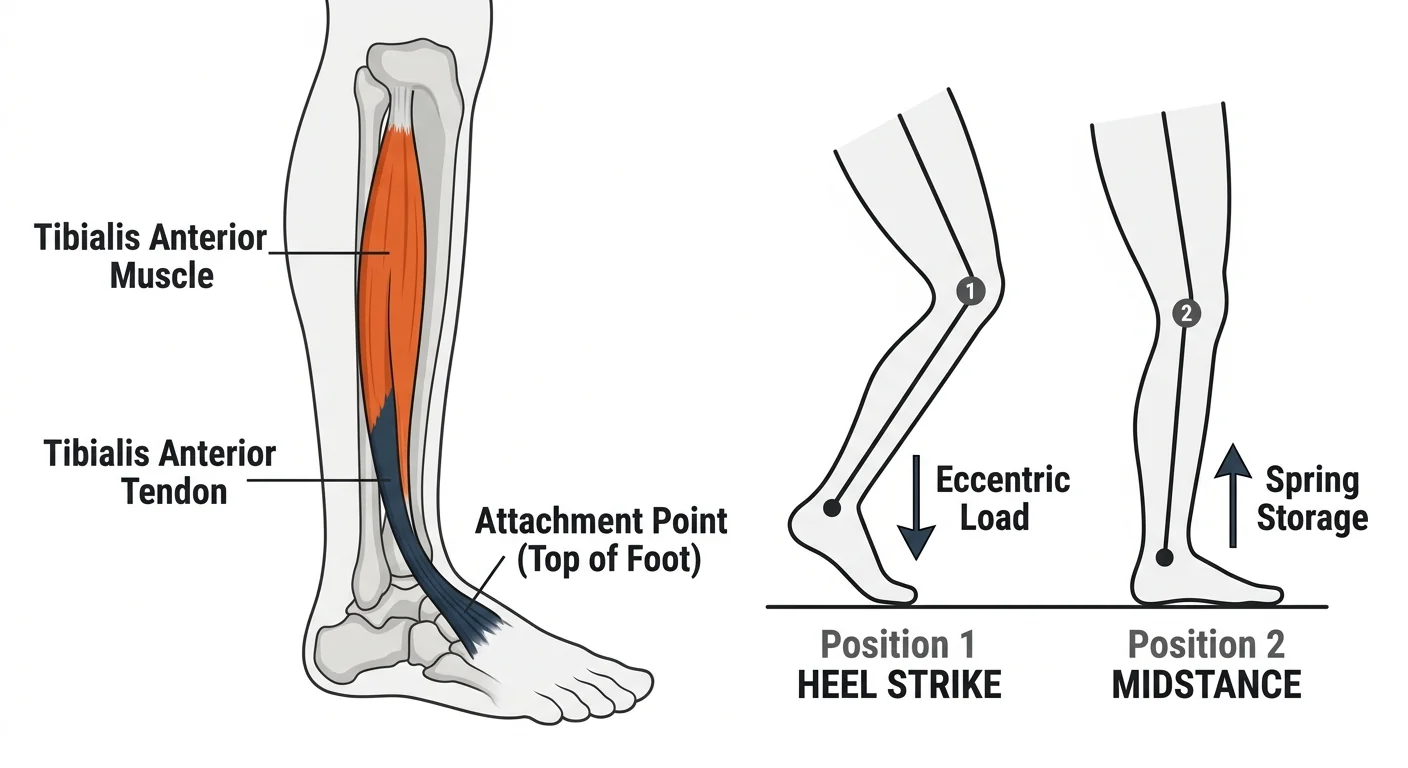
The tibialis anterior is a long muscle running down the outer edge of your shin bone, just outside the tibia.
Its tendon crosses the front of the ankle and attaches to the top of your foot, near the peak of your arch, giving it its primary function: pulling your foot up toward your knee, the motion called dorsiflexion.
During running, it carries out 2 important jobs at specific moments in the gait cycle.
At heelstrike, it contracts eccentrically, working while lengthening, to decelerate the rate at which your foot drops to the ground and slow the transition from heel contact to flat foot.
The tibialis anterior works hardest during the first fraction of a second after heel contact, absorbing the foot’s drop force before your foot reaches midstance.
At midstance, it shifts to a stabilizing role, stiffening the ankle so your foot and ankle can store and return energy like a spring.
Those 2 roles, eccentric deceleration at heelstrike and stiffening during midstance, are where most of the load on this tendon accumulates over a run.
Research has shown that in a study of over 2,000 injured runners tracked across 2 years, tibialis anterior tendonitis did not appear among the 26 most common running injuries, underscoring how specific the biomechanical conditions have to be for this injury to develop.

What Does Anterior Tibialis Tendonitis Feel Like?
The injury typically presents as a dull, aching pain along the front of the ankle or lower shin, tracing the path of the tibialis anterior tendon from the leg diagonally across the ankle.
Early in the injury, pain follows a familiar arc: it hurts at the start of a run, eases as you warm up, then returns toward the end.
As the condition worsens, pain shows up earlier in the run and takes longer to fade.
If the pain persists after your run, stiffens overnight, or wakes you up, the tendon is under more load than it can currently handle and the injury is progressing.
Some runners notice their foot on the injured side sounds louder at heelstrike, a slapping noise with each foot contact.
That’s the tibialis anterior reducing how forcefully it contracts to limit its exposure to the eccentric load, a natural protective response that signals the tendon is struggling.
You may also notice that pressing directly on the tendon, along the diagonal line crossing the front of the ankle, produces a distinct tenderness that differs from any bone-level pain.
How Do You Rule Out More Serious Causes of Anterior Shin Pain?
3 other conditions produce pain in roughly the same area and need to be excluded before you assume it’s the tibialis anterior tendon.
Lace Bite
Lace bite is aggravation along the front of the ankle caused by shoes laced too tightly, creating direct pressure on the extensor tendons and the tibialis anterior tendon below the lace line.
Loosen your laces and experiment with relacing to skip a crossing near the front of the ankle.
If pain eases within a day or two without any other change to your training, the culprit was your footwear.
Anterior Tibial Stress Fracture
An anterior tibial stress fracture is not the same as the more common medial shin stress fractures most runners know about.
It occurs on the leading edge of the shin bone, the front surface of the tibia, which is the tension side of the bone under load.
Anterior tibial stress fractures are considered high-risk because they occur on the tension side of the bone, meaning the fracture is pulled apart with each footstrike rather than compressed, which makes healing significantly slower.
The key differentiator is bone-level pain: a sharp, localized tenderness when you press directly on the front of the shin bone itself, not on the muscle or tendon alongside it.
If you have that kind of point tenderness on the bone, see a doctor before running again.
Exertional Compartment Syndrome
Exertional anterior compartment syndrome occurs when the fascial sheath surrounding the tibialis anterior muscle is too small to accommodate the muscle swelling that comes with increased blood flow during exercise.
Pressure builds inside the compartment, causing pain, and in more pronounced cases, numbness, tingling, or a full sensation inside the shin during or after a run.
These symptoms warrant a medical evaluation, because the definitive diagnostic test, a compartment pressure measurement during exercise, requires clinical access and rules out a condition that doesn’t respond to the same rehab as tendinopathy.
What Causes Anterior Tibialis Tendonitis in Runners?
Because the tibialis anterior works eccentrically at heelstrike on every single footstrike, the primary driver of tendinopathy is cumulative load, meaning any factor that increases how hard that deceleration phase works or reduces the tendon’s capacity to handle it.
The most common contributing factors in runners are:
- Rapid mileage increase. Tendon tissue adapts more slowly than muscle and cardiovascular fitness, so a jump in weekly mileage can outpace the tendon’s ability to remodel.
- High heel-to-toe drop footwear. A higher drop creates more mechanical leverage on the ankle at heelstrike, increasing the angular displacement the tibialis anterior must control during the transition from heel contact to flat foot.
- Hard training surfaces. Asphalt and concrete reduce the time window over which the foot drops after heelstrike, creating a steeper deceleration curve and a higher peak eccentric demand on the tendon.
- Pronounced heelstrike pattern. Runners with a heavy, overreaching heel strike place the foot farther in front of the center of mass, amplifying the drop speed and the eccentric load that follows.
Injury rarely comes from any single factor, but from a combination of them.
More miles on harder surfaces in higher-drop shoes is the most common cluster that pushes the tibialis anterior tendon past its capacity.
How Do You Treat Anterior Tibialis Tendonitis?
The treatment framework for tibialis anterior tendinopathy has 2 goals: reduce the load the tendon is exposed to while you run, and progressively build the tendon’s capacity to handle that load again.
Both have to happen simultaneously.
Cutting load alone doesn’t rehabilitate a tendon, and loading a tendon that’s still inflamed will delay recovery.
Reduce heel-to-toe drop.
Transitioning to shoes with a lower heel drop (4mm to 8mm) reduces the angular displacement at heelstrike that the tibialis anterior has to decelerate.
This is one of the most direct mechanical adjustments you can make, and it works best when done gradually over 3 to 4 weeks to avoid shifting load too quickly to the calf and Achilles.
Shift to softer surfaces.
Grass, gravel paths, or a rubberized track spreads the heelstrike impact over a slightly longer time window, reducing the peak rate of foot drop and the resulting eccentric demand on the tendon.
Kinesiology taping.
A single strip of kinesiology tape applied along the length of the tendon, starting at the midfoot and running up toward the lower shin, can partially offload the tendon by providing elastic support across the ankle joint.
Apply full tension to the section of tape that crosses the ankle to take advantage of the elastic properties of the tape.
Compression sleeves.
Calf sleeves or compression socks are worth trying, particularly for managing post-run stiffness.
The tactile feedback and mild compression can support the tendon during the early stages of recovery.
RunnersConnect Bonus
Download our Top 5 exercises to prevent anterior tibialis.
It’s a PDF with images and descriptions of the 5 most effective prevention and rehab exercises for runners with anterior tib issues.
What Are the Best Exercises for Anterior Tibialis Tendonitis?
Strengthening the tibialis anterior is the part of the rehab that most runners skip, and it’s the part that determines whether the injury comes back.
Evidence on tendinopathy management consistently shows that progressive loading, especially eccentric loading, drives tendon remodeling and restores tensile strength.
3 exercises address the tibialis anterior specifically, and none of them require equipment.
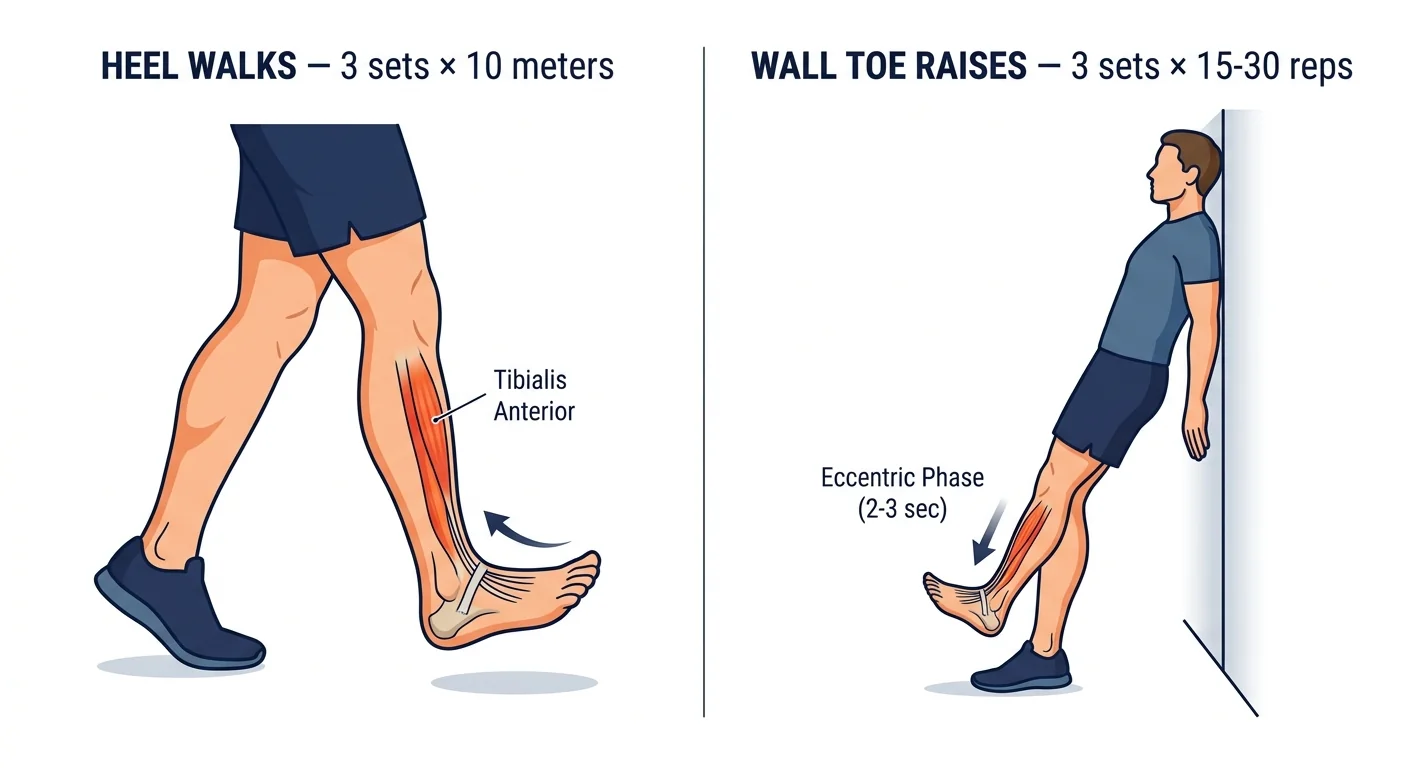
Heel Walks.
Remove your shoes and walk on your heels only, keeping your forefoot completely off the ground by actively dorsiflexing throughout each step.
Start with 3 sets of 10 meters with full recovery between sets, and add distance incrementally as strength improves.
Eccentric Wall Toe Raises.
Stand about 30cm from a wall and lean back until your shoulder blades rest lightly against it, with your ankles, knees, hips, and shoulders forming a straight diagonal line.
From this position, use your shin muscles to lift your forefoot off the ground, then slowly lower it back down over 2 to 3 seconds.
Start with 3 sets of 15 slow repetitions and 15 faster repetitions, building to 3 sets of 30 reps over several weeks.
The slow lowering phase is the eccentric component that promotes tendon remodeling.
Towel Toe Curls to Dorsiflexion.
Sit in a chair with a light towel on the floor under your foot.
Curl your toes to grip the towel, then actively lift your forefoot by dorsiflexing, working the tibialis anterior through its full range.
Start with 3 sets of 20 reps, adding a small weight on the towel as strength improves.
Mild muscle soreness in the shin muscle is expected when you start.
A spike in tendon pain at the injury site during the movement means the load is too high and you need to back off.
A 12-week clinical trial on eccentric loading for tendinopathy found that a heavy eccentric loading protocol produced substantially better return-to-activity rates than concentric-only training, establishing eccentric work as the foundation of tendinopathy rehab.
Can You Keep Running with Anterior Tibialis Tendonitis?
Running through this injury is possible for most runners, within clear pain thresholds.
Research using a pain monitoring model for tendinopathy management established that continued activity is safe as long as pain stays at or below 5 out of 10 on a scale where 10 is the worst pain you can imagine.
That threshold alone isn’t the full picture.
2 additional rules have to hold alongside it: pain must not be worse the day after a run than it was before, and it must not trend upward from week to week.
If either condition fails, reduce your run volume until both conditions are consistently met before increasing again.
Pain that worsens across consecutive training days or leaves residual tenderness the next morning is a signal to take 2 to 3 days completely off.
Recovery from tibialis anterior tendinopathy typically takes 4 to 8 weeks with consistent exercise and load management.
Runners who catch it early and adjust their footwear and surface tend to recover toward the shorter end of that range.
The injury rarely requires complete time off from running.
For a comparison on adjacent tendon injuries with a similar recovery approach, the posterior tibial tendonitis protocol follows the same pain-monitoring framework but targets the inside of the ankle.
| Treatment element | Goal | Starting protocol |
|---|---|---|
| Lower heel-drop shoes | Reduce eccentric demand at heelstrike | Transition gradually over 3 to 4 weeks |
| Softer running surfaces | Extend the time window of foot drop | Replace 50%+ of hard-surface miles |
| Heel walks | Strengthen tibialis anterior | 3 x 10m, progress distance weekly |
| Eccentric wall toe raises | Drive tendon remodeling | 3 x 15 slow + 15 fast, build to 3 x 30 |
| Kinesiology taping | Offload tendon during runs | Single strip with full tension at ankle |
| Pain monitoring | Determine when to run vs. rest | Pain at or below 5/10, no next-day spike |



2 Responses
John, great timing for this article since my tibialis anterior just started flaring up last week. After reading your post, I’m planning to focus on the strengthening aspect more since the rest/massage/anti-inflammatories aren’t doing much good so far. What are your thoughts on toe raises off a step, with assisted return to start, similar to your achilles rehab routine? This would potentially isolate the eccentric motion and avoid the weighted contraction. Also, I’ve found the elliptical to be good cross-training since it removes the plantar flexion from my stride.
Ah, this article has been the most helpful of many I’vebeen sifting through! I’m wondering if this is what I have. It’s just flared up for a second time, despite just taking a month off running because of it. Pain started both times directly where the tibialis anterior tendon lies. When I kept running on it before, the pain spread up where I think the actual muscle is, round to the anterior and more lateral side of the leg, making it painful to weight bear/walk on it. So I stopped running altogether for a month. Tried a couple of short test runs last week, felt fine, have gone back into normal running routine this week and its started again at the front of my ankle.
Does this mean I need to give up on running altogether for the a considerable amount of time?! It’s very frustrating!! I’ve also wondered whether being a more forefoot runner, (well, almost all up on the toes and leaning slightly forward, and living in a very hilly city) causes it as the ankle is in a more dorsi-flexed position?
Your article has explained it very clearly. Perhaps I just need to work on some strengthening exercises.