Training load drives 60-70% of all running-related injuries.
That one number changes how you should think about prevention.
Most running injuries are loading errors.
This guide covers each injury factor in order of the evidence supporting it, from the causes with the strongest research behind them to the interventions runners spend the most time on with the weakest return.
You’ll learn:
- Why training load causes most running injuries and the ratio that predicts risk
- How strength training cuts overuse injury risk by roughly half
- What cadence adjustments actually reduce impact forces during running
- When footwear matters and when it has no measurable effect on injury risk
- Red flags that mean you need a medical assessment, not more rest
- A pain-monitoring protocol for returning to running safely after time off
Why does training load cause most running injuries?
Your body adapts to running stress through a predictable cycle: load, recover, adapt.
When load increases faster than tissue can absorb and recover from it, something breaks down.

In practical terms, the danger zone is not high mileage.
It’s a sharp spike in mileage relative to what your body is used to handling.
A runner averaging 40 miles per week for six months can safely train at 45.
A runner finishing a 25-mile week and jumping to 40 is taking on a ratio well above 1.5.
The 10% rule, limiting weekly mileage increases to no more than 10% above the previous week, is a practical proxy for keeping your acute-to-chronic ratio in a safe range.
Keeping a simple training log is the most underused injury prevention tool available to non-elite runners.
You can’t perceive your accumulated load in real time, but you can see the pattern on paper before the next block starts.
Pain is worth reframing here too.
Pain is a warning signal from the nervous system that fires before structural damage has occurred, as a protective mechanism.
How much pain you feel does not accurately measure how much tissue damage has happened, which means fear of serious injury can amplify pain signals and understanding the mechanism behind pain can reduce them.
How does strength training lower your injury risk?
Getting stronger increases the load your muscles and tendons can absorb before reaching their failure threshold.
The same training volume creates less relative stress on a stronger runner’s body.
Running is a series of single-leg hops, each requiring your calf, quad, glute, and hip muscles to absorb and re-release ground contact force.
This process, called the stretch-shortening cycle, involves muscles and tendons storing elastic energy at landing and releasing it for propulsion.
The stiffer and stronger that spring, the less energy leaks out as injury-producing stress on bones, cartilage, and connective tissue.
Two strength sessions per week, built around single-leg movements, address this directly.
Bulgarian split squats, single-leg deadlifts, and eccentric calf raises load the muscles and tendons along the same mechanical pathways as running.
That specificity is why isolated gym exercises like leg press produce weaker injury prevention results than single-leg functional movements.
Strength training two days per week, focused on single-leg movements, is the most evidence-based injury prevention tool available after managing training load.
Stretching is a common substitute runners reach for instead.
Flexibility reduces the spring stiffness running requires, which can increase rather than decrease injury risk when it replaces strength work in a training week.
Stretching and mobility work have a legitimate role in recovery and warm-up routines.
The problem is when they substitute for the strength sessions that actually change the tissue’s load capacity.
Does your running technique affect injury risk?
Running technique determines which tissues absorb the most impact load at each footstrike.
Adjusting it can reduce stress on sensitized tissue during rehabilitation and lower specific injury risk over time.
Cadence is the most accessible gait variable to adjust without professional supervision.
Count your steps for 30 seconds during an easy run, multiply by 4, and you have your current steps per minute.
A cadence below 160-165 steps per minute at easy pace typically indicates low-frequency, high-impact mechanics.
Increasing that number by 5% is the target, using a metronome app during easy runs to anchor the new rhythm over 4-6 weeks.
Gait analysis focused on pronation category and footstrike prescription has not been shown to reduce injury rates in randomized controlled trials.
Technique adjustments are most valuable during injury rehabilitation: finding a running form that allows pain-free movement gives the nervous system a chance to recalibrate without the stimulus that caused the problem.
Overhauling technique as a standalone prevention strategy for an uninjured runner has weaker support in current research.
Does shoe choice prevent running injuries?
Shoe selection has a weaker influence on injury risk than training load, strength, and technique.
Different shoes do load tissues differently.
A higher heel drop shifts stress away from the Achilles and calf, which makes it a specific, targeted choice during Achilles tendinopathy rehabilitation.
A lower-stack shoe trains ground feel and foot proprioception for runners who want to build intrinsic foot strength.
These are targeted applications where shoe modification has a logical mechanism behind it.
The practice of categorizing runners into high, neutral, and flat arch types and prescribing stability or motion-control shoes based on pronation has not been validated by injury outcome research.
When choosing a shoe, comfort during a test run is the most reliable selection criterion available.
A shoe that fits comfortably from the first outing avoids the loading asymmetries that develop when a runner adapts movement patterns to accommodate discomfort.
What about stretching, foam rolling, and taping?
These tools occupy the top of the evidence hierarchy: useful in specific contexts, but a weak foundation for injury prevention.
Foam rolling reduces post-run muscle soreness and improves short-term tissue extensibility before a workout.
Stretching improves range of motion within a session but has no demonstrated effect on long-term injury rates.
Kinesiology tape provides proprioceptive feedback that runners find useful during rehabilitation from patellar tendinopathy and IT band issues, though the effect is largely mechanical and temporary.
Runners who treat foam rolling, stretching, or tape as primary interventions while ignoring training load or skipping strength work rarely resolve recurring injuries.
Used alongside proper load management and strength training, any of these tools can play a supporting role in a complete training week.
The issue is prioritization, not permission.
When should you see a doctor about a running injury?
Working through training load, strength, and technique is the right starting point for most running pain.
Certain symptoms bypass that checklist and require a sports medicine physician, physiotherapist, or orthopedic specialist without delay.
See a healthcare professional right away if you notice any of these:
- Sharp, localized bone pain that worsens with every footstrike, which can indicate bone stress injury
- Significant joint swelling that persists beyond 48 hours
- Numbness, tingling, or weakness in the foot or lower leg during or after running
- A sudden sharp pop followed by immediate pain and loss of function
- No improvement after two full weeks of reduced training load
Bone stress injuries require imaging for a confirmed diagnosis before returning to running, since symptoms alone can’t distinguish a stress reaction from a complete fracture risk.
If no red flags are present but pain has persisted beyond three weeks with reduced load, a physiotherapy assessment is still worth scheduling.
A good physiotherapist evaluates training load, strength gaps, and running mechanics, and often identifies contributing factors that are invisible without an outside assessment.
For nutritional support during injury recovery, RC’s guide on the best foods to eat while injured covers the evidence on what supports tissue repair.
RunnersConnect Bonus
Download your FREE Injury Assessment and Prediction Video now.
A good injury prevention program starts with assessing where you’re weak and where you might be tight or inhibited. In the video I’ll demonstrate the six mobility tests you need to perform to assess what you need to begin working on.
How do you return to running after an injury?
The most common reason a resolved injury turns chronic is returning to full training before healing tissue is ready to handle the load.
The principle governing a safe return is the same one governing training load management: increase no faster than healing tissue can absorb.
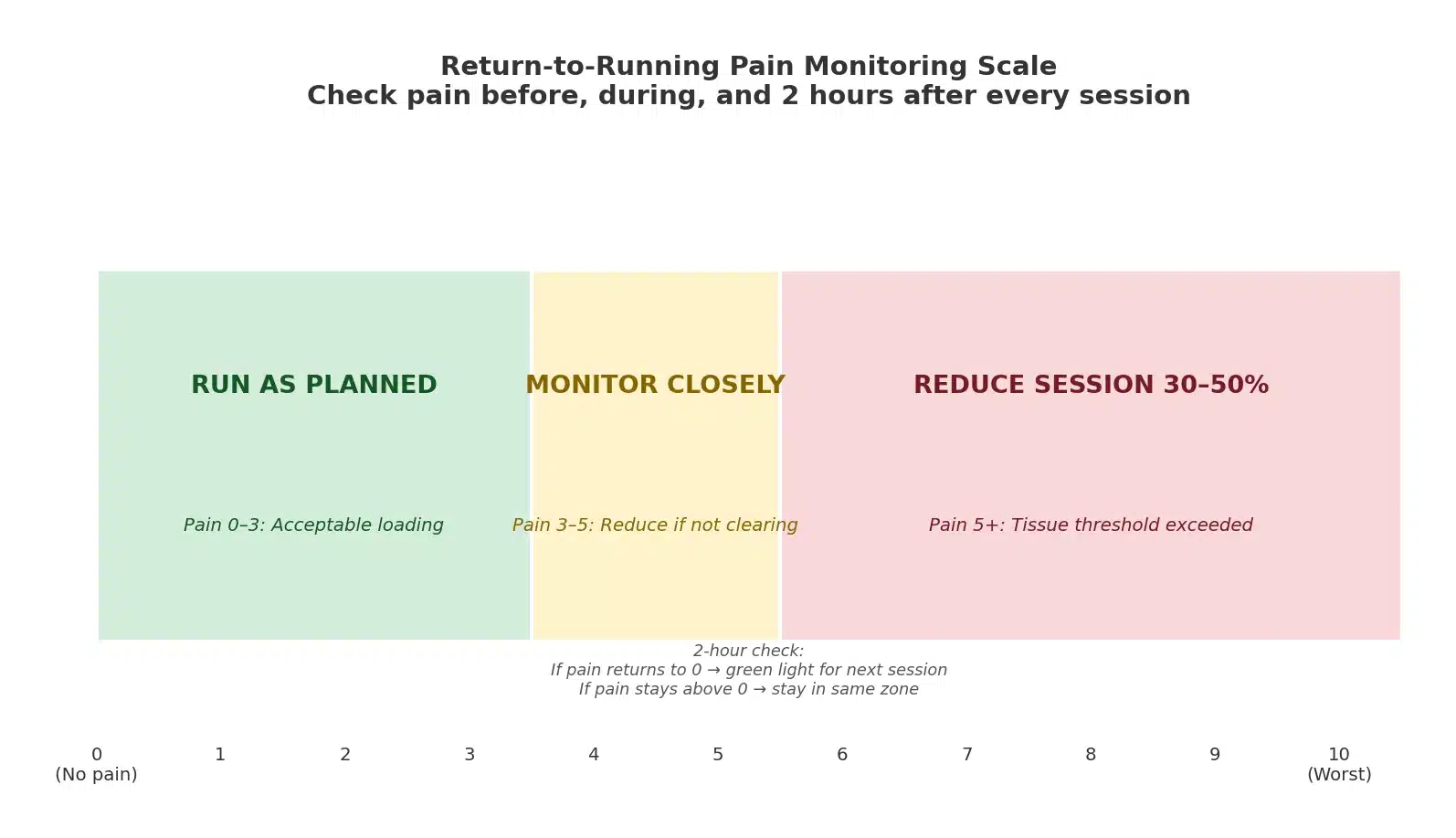
A reliable method for guiding that process is pain monitoring on a 0-10 scale, tracked before, during, and two hours after each run.
Pain of 3 or below during a session means tissue is being loaded within its current tolerance.
Pain above 5 during a run, or pain that stays elevated two hours after finishing, is a signal to cut the next session by 30-50%.
Pain returning to 0 within two hours of finishing is a green light to maintain planned progression the following day.
For every week spent unable to run, plan one week of careful re-introduction before returning to full training volume.
Cross-training fills the aerobic gap during this period without the ground reaction forces that stressed the injured tissue.
Pool running and cycling are the most effective options for maintaining cardiovascular fitness while the tissue heals.
For a step-by-step return framework, RC’s full guide on returning to running after an injury covers the detailed weekly protocol.
| Factor | Evidence Strength | Effect on Injury Risk | Practical Action |
|---|---|---|---|
| Training load management | Very strong | Drives 60-70% of injuries when mismanaged | Keep weekly increases at 10% or below; track ACWR |
| Strength training | Strong | Reduces overuse injury risk by roughly half | 2 sessions per week, single-leg movements |
| Running technique (cadence) | Moderate | 5-10% cadence increase reduces ground forces | Count steps per minute; use a metronome app |
| Footwear selection | Weak to moderate | Shoe type has no proven effect on injury rates | Select for comfort; use targeted modifications during rehab |
| Stretching / foam rolling / tape | Weak | No measurable effect on long-term injury rates | Supporting role in recovery; not primary prevention |
In Summary
Most running injuries are solvable and most are preventable when you address causes in order of evidence.
Training load first.
Strength second.
Running technique third.
Footwear, foam rolling, and recovery tools after that, used where they have a specific mechanism, not as primary prevention strategies.
Runners who stay injured for months are usually spending time at the top of the evidence hierarchy while ignoring the bottom of it.
Getting the fundamentals right is rarely the exciting answer, but it is what the research consistently support