

Sharp pain along the inner side of your ankle.
A dull ache that creeps up your shin after a few miles.
Tenderness when you push on the tendon just below that bony bump on the inside of your ankle.
If any of that sounds familiar, you may have posterior tibial tendon dysfunction, one of the most underestimated injuries in running.
Most runners try to run through it. That’s the wrong call.
This is the one injury where pushing through can permanently change the shape of your foot.
The good news: catch it early and follow a structured protocol, and full recovery is absolutely possible without surgery.
In this guide, you’ll learn:
- Exactly what the posterior tibial tendon does and why it fails in runners
- How to self-diagnose using a simple at-home test
- Why this injury progresses in stages, and what each stage means for your treatment options
- The 4-component treatment framework backed by clinical research
- A week-by-week rehab exercise progression you can follow at home
- When it’s safe to start running again
RunnersConnect Bonus
Download our Posterior Tibial Injury Outline for free.
It’s a PDF with the conservative and aggressive treatment options for runners suffering from posterior tibial tendon pain.
What Is the Posterior Tibial Tendon?
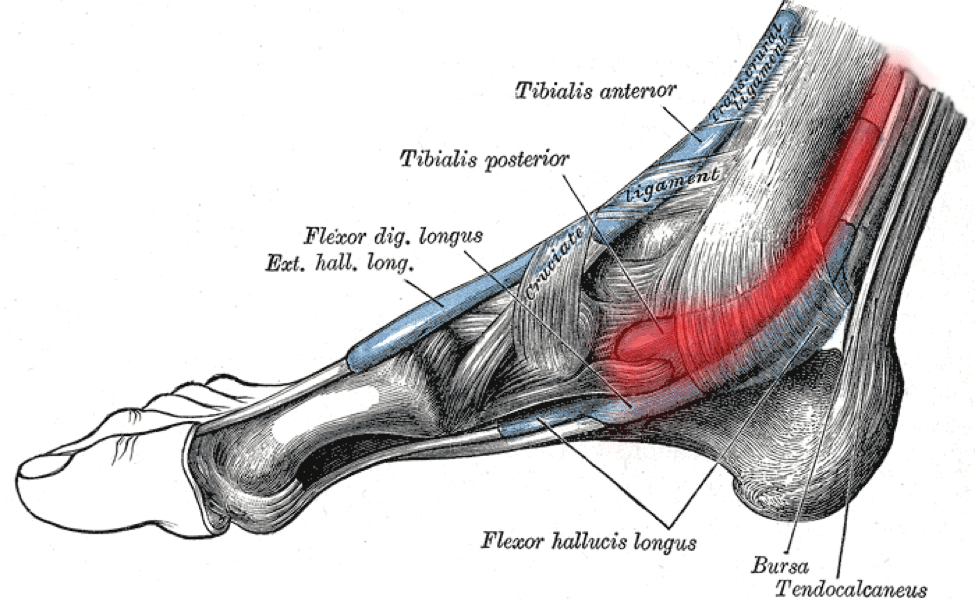
The posterior tibial tendon runs up the inside of your ankle, connecting the tibialis posterior muscle (buried deep in your calf) to the bones in the arch of your foot.
The tendon itself is no thicker than a pencil. But its job is enormous.
Every time your foot hits the ground and pushes off, the posterior tibial tendon locks your ankle in place and maintains your arch in a rigid, stable position.
Without it, your arch collapses under load, your ankle rolls inward, and the rest of your lower leg has to compensate.
Think of your foot’s arch as a suspension bridge. The posterior tibial tendon is the main cable holding tension.
If that cable weakens or tears, the bridge sags.
In advanced cases of posterior tibial tendon dysfunction, the arch collapses permanently.
How Do You Know If You Have Posterior Tibial Tendonitis?
The hallmark symptom is pain along the inside of your ankle and foot, sometimes extending a few inches up your shin.
There may be mild swelling, and the area will usually be sore to press directly on the tendon.
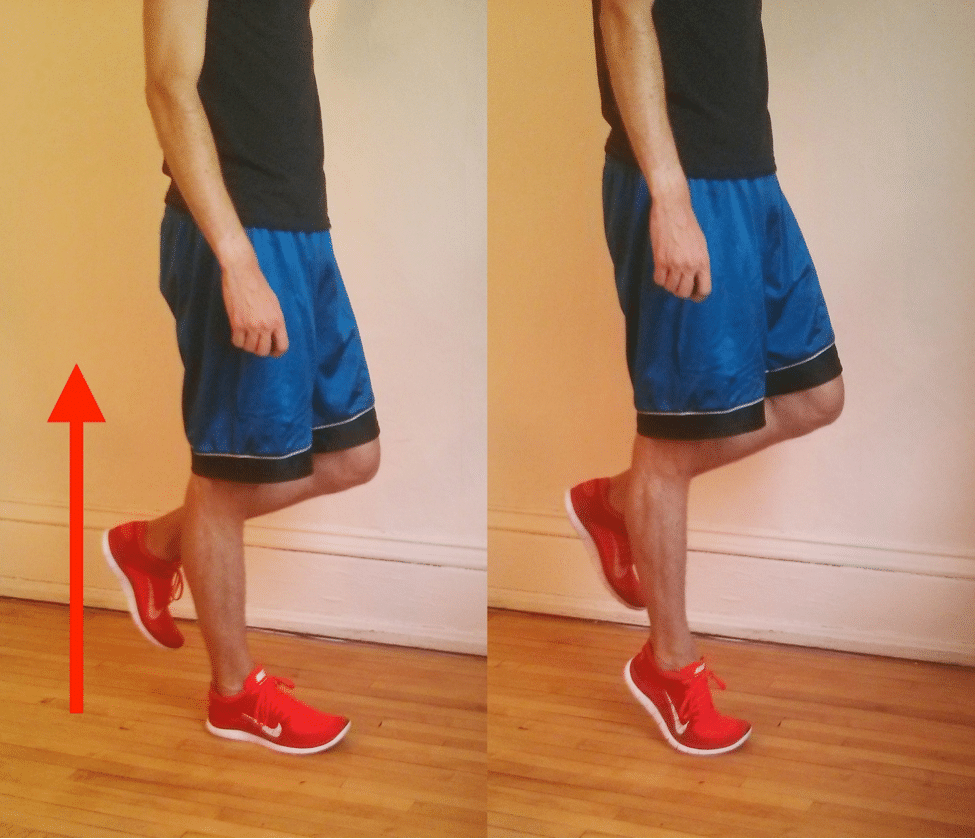
The most reliable self-test is the single-leg heel raise.
Stand on the affected leg with your knee straight. Rise up onto the ball of your foot as high as you can go, reaching full plantarflexion at the top.
Hold for a second, then lower slowly.
Pain or weakness along the inside of your ankle during this test is the clearest indicator of posterior tibial tendon dysfunction.
In more severe cases, you won’t be able to rise onto your forefoot at all.
Studies have used this test as an inclusion criterion for posterior tibial tendon dysfunction research, which tells you how specific it is.
It also helps rule out similar injuries. Medial tibial stress syndrome (shin splints) and stress fractures of the medial malleolus can cause pain in the same region but won’t produce ankle weakness on the heel raise test.
Why You Can’t Just Run Through This
In a case-control analysis of 2,002 running injuries, posterior tibial tendon dysfunction ranked 26th: relatively uncommon.
What makes it dangerous is the potential for permanent progression.
Research has shown that the posterior tibial tendon has a zone of relative avascularity in the critical section wrapping around the medial malleolus, which is why it heals far more slowly than most soft tissue injuries.
Running on an injured posterior tibial tendon adds damage to a structure that already can’t repair itself fast enough.
As the tendon weakens, your arch drops and your foot pronates more under load. That increased pronation puts more stress on the posterior tibial tendon.
More stress means more damage. More damage means more pronation.
The cycle repeats until, in severe cases, the arch collapses permanently.
The 4 Clinical Stages
Doctors classify posterior tibial tendon dysfunction in 4 progressive stages. Knowing your stage determines your treatment options.
Stage I: Tendon inflammation or microdamage, but no change in foot shape. Conservative treatment works well.
This is where you want to catch it.
Stage II: The tendon begins to elongate and the arch gradually flattens. At this stage, most patients can no longer complete a single-leg heel raise.
Conservative treatment is still possible but requires more intensive management, often with specialized ankle-foot orthoses.
Stages III and IV: Partial or complete tendon rupture with permanent foot and ankle deformity. Surgery is usually required.
The treatment protocol below applies to Stage I. If you are in Stage II or beyond, see a podiatrist or foot and ankle orthopedist before starting any rehab program.
What Causes Posterior Tibial Tendonitis in Runners?
The most common cause is classic overuse: ramping mileage too fast, or resuming training too quickly after time off.
Acute tears from a fall or sudden ankle roll are less common but do occur.
Runners with a naturally high arch may carry some protection, since the tendon doesn’t have to work as hard to maintain the arch. Runners of every arch type still develop this injury, though.
In the general population, it’s most common in overweight, middle-aged women. Among runners, the pattern flips: a 2002 review of over 2,000 injured runners found it more common in men than women.
The honest answer is that the risk profile for runners specifically isn’t well understood.
What Does the Treatment Protocol for Posterior Tibial Tendonitis Look Like?
The research on conservative treatment points consistently to 4 key components working together. No single piece works in isolation.
- Reduce load on the tendon
- Support the arch with appropriate footwear and orthotics
- Stretch the calf complex
- Progressively strengthen the tendon and surrounding structures
Below is how to execute each one.
RunnersConnect Bonus
Download our free Posterior Tibial Injury Outline, a PDF with conservative and aggressive treatment options, mapped out clearly for runners.
Step 1: How Do You Reduce Load on the Tendon?
Stop running. Yes, completely.
The posterior tibial tendon heals slowly because of poor blood supply to the section wrapping around your medial malleolus. Running adds damage to a structure that can’t repair itself fast enough to keep pace.
Swimming and cycling are generally safe as long as they’re pain-free. Aqua jogging is particularly well-suited for this injury (more on that below).
Keep daily walking to a minimum as well, especially on uneven surfaces.
The goal during this phase is giving the tendon enough of a break to actually start healing before you ask it to do rehab work.
Step 2: What Shoes and Orthotics Do You Need?
Every clinical study that has successfully treated posterior tibial tendon dysfunction with conservative measures used arch support as a component of the protocol.
The goal is to reduce the mechanical demand on a tendon that can’t currently handle full load.
Arch support does this by propping up the arch so the posterior tibial tendon doesn’t have to work as hard with every step.
One study asked patients to wear shoes and orthotics for at least 90% of their waking hours, including around the house.
That’s not an exaggeration. Walking barefoot on hard floors still stresses the tendon.
Wear your shoes from the moment you get up.

On the question of custom vs. over-the-counter: for plantar fasciitis and some other foot injuries, rigid OTC orthotics (like Superfeet or PowerStep) have been shown to work just as well as custom-made ones. For posterior tibial tendon dysfunction, that comparison hasn’t been studied.
What the research supports is that some arch support is clearly better than none.
Whether you need custom orthotics is a question for your podiatrist or orthopedist. See our full breakdown of the science behind custom orthotics for what to expect from that conversation.
Step 3: How Should You Stretch Your Calves?
Three separate clinical studies that successfully treated posterior tibial tendon dysfunction included a structured calf-stretching protocol.
The standard protocol:
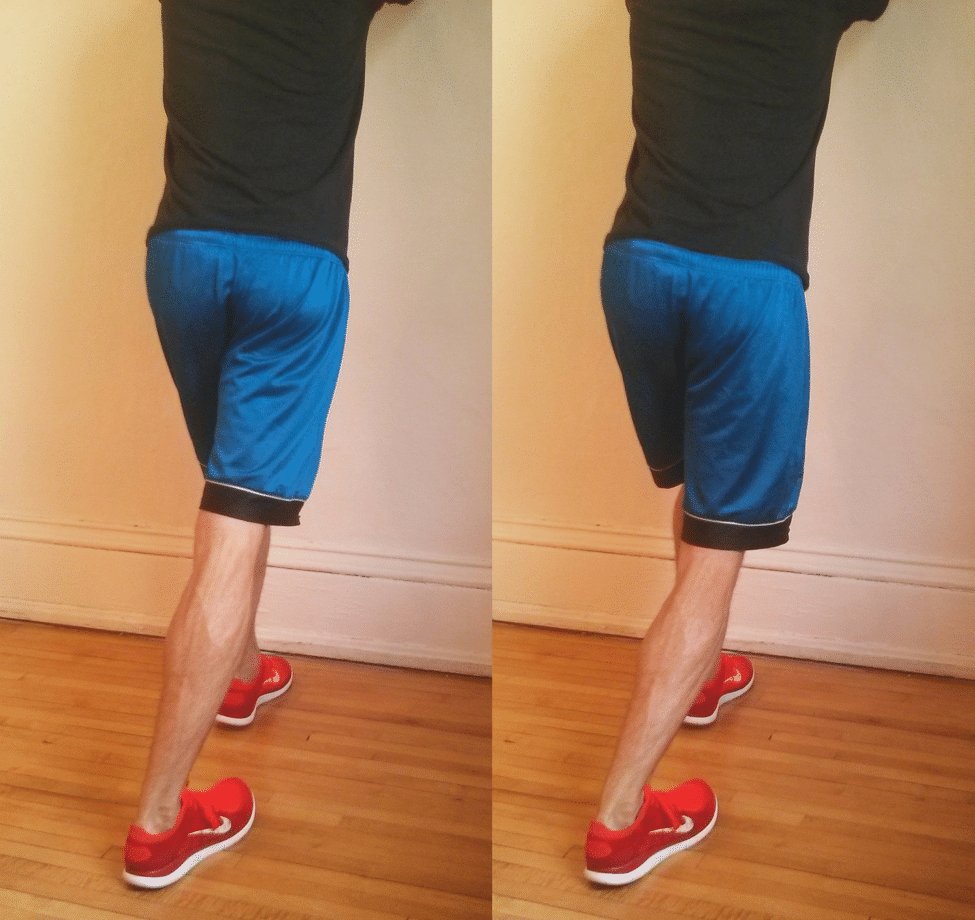
- 3 sets x 30 seconds of a wall calf stretch with a straight knee (targeting the gastrocnemius)
- 3 sets x 30 seconds with a bent knee (targeting the soleus)
- Done twice per day, on both legs
- Use an incline board if you have one, as it deepens the stretch
One important detail from Kulig et al.’s 2009 USC study: do all your stretching in your shoes and orthotics.
The support changes the mechanics of the stretch in a way that’s relevant to tendon loading.
Step 4: What Exercises Should You Do for Posterior Tibial Tendon Rehab?
This is where the research gets specific, and where most informal advice falls short.
A 2006 paper by Alvarez et al. at the University of Tennessee laid out a detailed 16-week conservative rehab program for Stage I posterior tibial tendon dysfunction.
A 2009 study by Kulig et al. at USC added a targeted eccentric loading component.
The protocol has 2 phases. Don’t jump to Phase 2 until you’ve completed at least 3 weeks of Phase 1.
Phase 1: Build Endurance (Weeks 1-3)
All exercises are done in shoes and orthotics. Stop if you feel significant pain.
Working into pain is not appropriate here.
Seated sole-to-sole exercise: Sit with your feet on the floor. Press the inside edges of your feet together and hold briefly, then release.
Start at 4 sets of 25 reps daily. Over 2 weeks, build to 12 sets of 25.
Then begin combining sets until you can do 300 continuous reps without stopping.
Theraband dorsiflexion (1x/day, 200 reps): Loop a theraband around the top of your foot and anchor it in front of you. Pull your toes up toward your shin against resistance.
Put a towel under your foot for smoother motion. Progress to a stronger band once 200 reps feels easy.
Theraband inversion, endurance (1x/day, 200 reps): Anchor the band at 45 degrees relative to your foot. Roll your foot inward (inversion) against resistance.
Towel under foot. Don’t rotate your leg.
All movement from the ankle.
Theraband eversion (1x/day, 200 reps): Same setup as inversion but rolling the foot outward. Towel under foot, band at 45 degrees.
Theraband inversion, strength (2x/day, 3 sets of 15): Same inversion movement, but with the heaviest theraband you can tolerate for 15 controlled reps.
Done twice daily. Perform slowly in both directions.
Increase resistance over time.
Phase 2: Functional Loading (Week 4+)
Add these once you’ve completed at least 3 weeks of Phase 1 without pain. All are done once daily, in shoes and orthotics.
Single-leg heel raises: Stand on the affected leg, rise up onto your forefoot, lower slowly. Start with just a few reps and build progressively to 50 continuous reps.
Use a wall lightly for balance, not for support.
Toe walking: Walk forward on your toes with heels fully off the ground. Start at 8-10 yards and build over time to 100 continuous yards.
Balance board tapping: Stand on your affected leg on a balance board. Tap the board to the ground in one direction, return to balanced position.
Repeat 20 times in each of 5 directions (forward, back, left diagonal, right diagonal, rotational). Then repeat the full sequence in reverse for a total of 2 sets of 20 in each direction.
Plan on 3 months of daily work across both phases.
Alvarez et al.’s full program ran 16 weeks, including an initial 2-week rest period. Kulig et al.’s protocols ran 10-12 weeks.
What Other Treatments Help Posterior Tibial Tendonitis?
Icing: Ice regularly, especially after rehab exercises. A common protocol is 10 minutes of ice massage with an ice cup, 10 minutes of rest, then another 10 minutes.
You can ice as often as every 2 hours.
Foam rolling your calves: Loosening your calf tissue reduces the tension transmitted to the posterior tibial tendon. Foam rolling is a useful daily addition alongside the stretching protocol.
Physical therapy: If you’re not improving after 6-8 weeks of consistent conservative treatment, a PT who works with runners can assess whether additional strength or flexibility deficits are contributing to the dysfunction.
Surgery: If months of conservative treatment haven’t helped, consult with a podiatrist or foot and ankle orthopedist who specializes in runners. There are many surgical options, and outcomes vary considerably by technique and provider experience.
Conservative vs. Aggressive Treatment: What Should You Try First?
Conservative (start here):
- Wear supportive shoes and orthotics at least 90% of waking hours, including at home
- Calf stretching: 3×30 seconds, straight and bent knee, both legs, twice daily
- Phase 1 theraband program: sole-to-sole, dorsiflexion, inversion (endurance + strength), eversion, daily for at least 3 weeks
- Phase 2 functional program: single-leg heel raises (build to 50), toe walking (build to 100 yards), balance board tapping, once daily after 3 weeks of Phase 1
- Ice after exercises, up to every 2 hours as needed
Aggressive (when conservative isn’t enough):
- Custom orthotics from a podiatrist or foot/ankle orthopedist
- Physical therapy for a personalized program and hands-on treatment
- Surgical consultation if Stage II or beyond, or if conservative treatment has failed after several months
What Cross-Training Can You Do With Posterior Tibial Tendonitis?
You don’t have to lose fitness while you recover.
Aqua jogging is the best option for this injury. It closely mimics running mechanics with zero impact on the posterior tibial tendon.
Research has found that runners who trained exclusively with deep water running for 4-6 weeks showed no measurable decline in 5k performance, VO2 max, lactate threshold, or body composition compared to runners who continued overland training.
Cycling and swimming are reasonable alternatives if aqua jogging isn’t accessible.
The key rule: whatever you choose should be completely pain-free. Any cross-training activity that loads the posterior tibial tendon directly needs to come off the list.
For more on how to structure your cross-training and which options work best for different injury types, see our guide on the best cross-training for injured runners.
When Can You Return to Running After Posterior Tibial Tendonitis?
No published research offers a specific return-to-running timeline for posterior tibial tendon dysfunction.
What the research does tell you is that this tendon has a tendency toward permanent damage if you rush it.
Only attempt a return to running after you can complete 50 single-leg heel raises without pain.
Start with very short, easy runs only. If any pain returns during or after a run, back off immediately.
Build up over several weeks before adding any pace or volume.
A physical therapist with distance running experience can help you build an individualized return-to-run plan, especially useful if you’ve had a longer or more complicated recovery.

18 Responses
I struggled with PTT for years, and it ultimately ended my collegiate career. I finally overcame it years later with a combination of orthotics, clamshell strengthening, topical anti inflammatories, and support shoes. But the key was finding a good self massage technique. Slowly rotating the foot while working my thumbs up the tendon and muscle behind the ankle bone and up the shin finally got everything to relax.
Thanks for sharing Stuart!
I enjoyed reading this article and i have developed this injury (that i have never had before,even from running on the treadmill,too fast for too long)..I cycle much more than running,because i was cycling between 16 and 32 miles everyday for work and.I changed my job to a local job and i wasn’t doing all the cycling mileage everyday and two weeks ago i used my turbo trainer on my bike and cycled at 22 mph for 20 mins doing this three times,so 1 hour cycling at 22 mph. That was enough to give me this injury for the first time .I have learnt more valuable lessons from doing too much exercise,too fast for too long!!!.Also look how quickly my fitness from cycling 16 to 32 miles everyday to only cycling 4 miles to work everyday dropped my fitness like a stone and that is why i have got this injury when i cycled for 1 hour at 22mph after six weeks of only cycling 4 miles a day.I am just going to rest,rest and more rest until this injury has gone and then have to build up my cycling fitness again.I can lift my left heel with a little soreness,so i guess i’m still ok to make a full recovery with rest over time,i hope so.Thanks Bruce
Mine is a longitudinal tear of the peroneal brevis tendon–the stabilizing tendon on the outside of the foot. Would these healing protocols work for me also? Thank you.
Hi Derrick, yes, many of the exercises we recommend throughout our posts are helpful for a variety of different injuries as they are strengthening all the muscles around the lower leg to prevent future injuries of all kinds. You may also want to check this one to out to make sure it is not weakness in your hip that is causing this injury https://runnersconnect.net/running-injury-prevention/the-relationship-between-hip-strength-and-running-injuries-the-latest-research/ Hope this helps!
Hi Coach Tina , I have PTT and a doc I went to see is recommending EPAT therapy. I don’t know of anyone that has done this so I am trying to get a perspective on this treatment to see if it worthwhile or not. I know it is relatively new ,but I dont want to waste $300.00 per treatment (3 are recommended) if it is just a scam treatment or hasn’t produced results for anyone else. Any advice you or anyone can offer me on this treatment ?
Thank you for this information on how to treat post. tib issues. For 8 months, I have been aching from what my new podiatrist thinks is an inflamed post. tib tendon being impinged by a talus that is rotated 40 or so degrees medically plus a torn, chronically sprained deep deltoid ligaments. I have tried two rounds of physical therapy totaling about 4 months, several injections including PRP and steroids, and significant reductions in my activity. It took me a few months to stop running entirely (I am obsessed running!). Finally I am non-weight-baring on my injured foot (just started week three of that). Do you have any conjectures on whether complete rest will finally help reduce my pain? I am also open to any additional advice you are willing to provide on how to treat this nagging injury. Finally, my advice for anyone with this injury is to stop running immediately.
Hi Katie. I realize it’s been a while since you posted. But I’m reaching out to you because I have the same problems. Are you available to chat on our similar conditions.? Mark
I, too, have been suffering from PTT for over 8 months. It has completely stopped my running. I kept thinking it was getting better so I would try to run again only to have it flare up but even worse. Now I am unable to run at all. I just completed 6 weeks of total rest, wearing an Aircast and using crutches. It did start to feel a little better but the swelling remains and the soreness is returning now that I am weight bearing again. Not sure what options that I have now other than surgery. I have found that few therapists understand this injury and more often than not they make the problem worse. I have been using topical anti inflammatory gel (Voltaren) but not sure it has made any difference. If anyone has any ideas let me know! This is a very frustrating injury and there is no quick fix, at least for me.
Hello, I am also suffering from this problem and my doctor advise is surgery. however the process seems worse then the problem it self.
i believe before going to these extreme one should try self healing. it is base on faith and the ability the body have to heal it self though faith in God.
As a follow up to my own post, it has now been 13 months dealing with this injury and it’s finally getting better. I am not running but I can now do all other activities with very little pain. I recently visited a great doctor at the Mayo Clinic. He is a sports orthopedic doctor. He talked to me about the Alfredson Protocol. Developed for Achilles injuries, it can be applied to this tendon. It focuses on strengthening the tendon while elongating it versus contraction exercises. It works. Google this. Respond if you’d like any more information. Good luck!
Hi, I don’t see a description of the “sole to sole” exercise. What is this?
Help! For 10 years I have had PTT issues. Dr. says that I no longer have a tendon-that it must have snapped. Who knows why. Not overweight and don’t really exercise or anything that would have strained it. I still have a high arch-always have. I wear orthotics and a brace. Sometimes I question the whole thing. This article talks about the foot becoming pronated and the arch falling. I have neither issue. I can’t stand on one foot on that foot and the foot is somewhat inward facing at the ankle. Going to go to a new doctor soon. This doctor made an Arizona brace for me, but come on! Who is going to wear that thing? It doesn’t even fit in a gym shoe and I have a professional job where I couldn’t wear gym shoes. Anyone ever hear of a PTT just snapping? Dr. says MRI shows that the tendon is missing. Anyone have any insight into a disappearing PTT? My issues seem different than the ones in the article and the comments.
Thank you for this informative post that finally revealed what I’ve been experiencing all these years. I’m not sure if I was born with this, but as a kid I would sometimes stretch after waking, and my foot would suddenly ‘lock’ with a sharp and intense pain. Only by pressing and rubbing the arch of my foot was I able to relax it. And I had no idea it’s related to the reason why my feet hurts after standing for long periods in the recent years. I’m gonna try those stretching exercises.
I may have early stage of this injury. My question is how do I know if it is posterior tibial tendonitis or the flexor hallucis longus? Are the treatments the same? When it first started I researched it a bit, started icing, and put my “good feet” arch supports in my work shoes. I plan on beginning this rehab regimen. Last thing I want is a flat arch!
Help please. i have ptti. my orthotic specialist has put a wedge in the medial forefoot region . Should it be placed in posterior(hindfoot,by calcaneus or forefoot?-
Dr Barry Shapiro
bps1@rogers.com
Chris said:
I’m in my 80’s, and although I’m not a runner I have been very active outdoors throughout my life. However, after a series of incidents since childhood, I now realize that earlier diagnoses as Plantar Fasciitis were hasty and incorrect, and that what I really have is Posterior Tibial Tendonitis! Now, I’m very pleased to have this information and the treatments provided on your website. For many years I’ve practiced a modified form of Trigger Point Therapy, and the patterns of pink and redness induced during my very brief treatment sessions match some of the illustrations shown on your pages. Thank you!
Feel free to delete this comment, but a chunk of this article above is repeated, which makes for tricky reading until you realize you can keep scrolling to get to the rest. It would be good to fix.