

We often hear about how running is “all about the hips”, and how the source of all your running injuries is weakness in the muscles around your hips, but what does that mean?
Which hip muscles are so critical to success as a runner?
Turns out your hip adductor and abductor muscles are a huge part of you being able to stay healthy as a runner, and if they are neglected, you are putting yourself at serious risk of an injury.
We are here to show you why this is the case, and what you need to do to make sure your hip abductors are strong to prevent future issues.
In the article Proper Running Form: Does Gravity Help You Run Faster?, we considered the importance of hip extension in running, and noted that in cases of runners with restricted mobility in the front of the hips (e.g. tight Quads and/or Psoas), we often see a forward drop of the pelvis, highlighted by an increase in the curve of the lower back.
What does that mean?
In other words, the body succeeds in traveling over the supporting leg, but without making optimum use of the powerful Gluteus maximus (the main muscle of the buttock).
As a result, stride length becomes compromised, propulsion is reduced, overall effectiveness of the running gait cycle is inhibited and risk of injury potentially raised.
This week’s article focuses on a smaller but equally important member of the glute family – the Gluteus medium. We are going to show you why the gluteus medius is important, and give you the best hip (and glute) strengthening exercises for runners that will help to stop your hip drop and keep you healthy.
No more of those tight hips! Ready to get started?
What is the Gluteus Medius and Why is it Important?
As can be seen in the image to the right (posterior view), the Gluteus medius or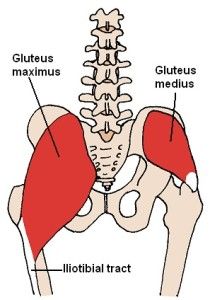 iginates at the dorsal ilium (uppermost, largest bone of the pelvis) below the iliac crest and inserts at the top outside surfaces of the greater trochanter (top of the thigh bone).
iginates at the dorsal ilium (uppermost, largest bone of the pelvis) below the iliac crest and inserts at the top outside surfaces of the greater trochanter (top of the thigh bone).
It is the major abductor of the thigh (moves the leg away from the midline of the body). The anterior fibers rotate the hip internally and the posterior fibers rotate the hip externally.
Whilst the Gluteus maximus is a hip extensor (moves your leg behind you) and is involved in the forwards & backwards tilting of the pelvis (dynamic stabilization in the sagittal plane), the Glute medius is a hip abductor (moves the leg out to the side) that plays a major role in controlling the sideways tilting of the pelvis.
Here’s the deal:
The Trendelenburg gait is exhibited by a person who through weakness in the abductor muscles, cannot maintain sufficient height of the opposite side of the pelvis to raise the foot and transfer weight to the other leg.
Instead, the pelvis drops downwards, meaning the affected person has to bend their leg more than usual at the knee in order to make up for the lack of lift.
To compensate, the stride on the unaffected side typically becomes shorter, along with a tendency for the person to lurch towards the weakened side in an attempt to maintain a level pelvis.
Does Weakness in the Hip Muscles Cause “The Hip Drop”
You might be wondering:
The term hip drop has become increasingly popular in articles today. It seems almost every runner has some level of it, and what does that even mean anyway?
In the diagram below, the drawings (A) and (B) illustrate a runner in left leg “swing phase”, meaning the left leg is off the ground and in the process of travelling forwards. The right leg is in mid-stance directly under the hips and taking maximum load as the body weight passes over it.
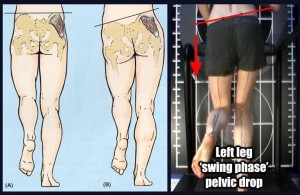
The Gluteus medius is highlighted as the dark area on the right hip.
Here’s the difference:
In image (A), the Gluteus medius is performing its role of dynamically stabilizing the pelvis such that the left hip does not drop more than 5 degrees (the image shows a straight line but in reality 4-5 degrees is regarded as the range necessary for minimizing vertical displacement of the body’s centre of gravity).
However, image (B) shows a weaker Gluteus medius not fulfilling its role and in effect allowing a marked drop (more than 5 degrees) of the left hip. The photo to the right of the drawings shows this same scenario for a real life runner.
What Does a Weak Gluteus Medius do?
Various studies have shown a link between Gluteus medius weakness and athletic injury:
- In a study by Fredericson et al (2000), 24 distance runners with Iliotibial Band Syndrome had the hip abductor strength of their injured limb compared to that of the non injured limb (and to that of a control group). It was found that on average Gluteus medius strength was 2% less on the injured side.
- After a six-week rehabilitation period with particular focus on strengthening the Gluteus medius (side-lying hip abduction and pelvic drops), 22 of the 24 injured athletes were pain-free and able to return to running. Furthermore, a six-month follow-up showed no reports of recurrence.
- Other studies have also linked weaker hip abductors and external rotators to Patellofemoral Pain Syndrome (Ireland et al.,2003; Robinson et al.,2007; Cichanowski et al.,2007).
How do I strengthen my gluteus medius?
Given the body’s remarkable ability to find and adopt a compensatory movement pattern when faced with weakness or dysfunction, it is very important to use a gradual, progressive exercise program when attempting to strengthen and stimulate use of a weak muscle/muscle group.
RunnersConnect Insider Bonus
Download your FREE Hip Strengthening Exercises Guide inside your Insider Members area.
Download a video and PDF version of the 5 most effective hip exercises for runners. You’ll get more images, full descriptions on how to perform and a video to help guide you.
Not a RunnersConnect Insider member? It’s FREE to join. Click here to get started
Though in recent years much attention has been given to the importance of “functional” exercise (i.e. one that mimics as much as possible the dynamic movement we are aiming to achieve), experience shows that giving the body too complex a movement pattern too soon can often hinder or prevent recruitment of the target muscle/muscle group.
Now:
Studies that quantify the electromyographic activity (EMG) of the Gluteus medius during common therapeutic rehabilitation also seem to support the use of exercises that some would dismiss as not “functional” enough. In the table below, collated values are shown for exercises that scored significantly in three such studies: Bolgla et al.,(2004), DiStefano et al.,(2009) and Boren et al.,(2011).
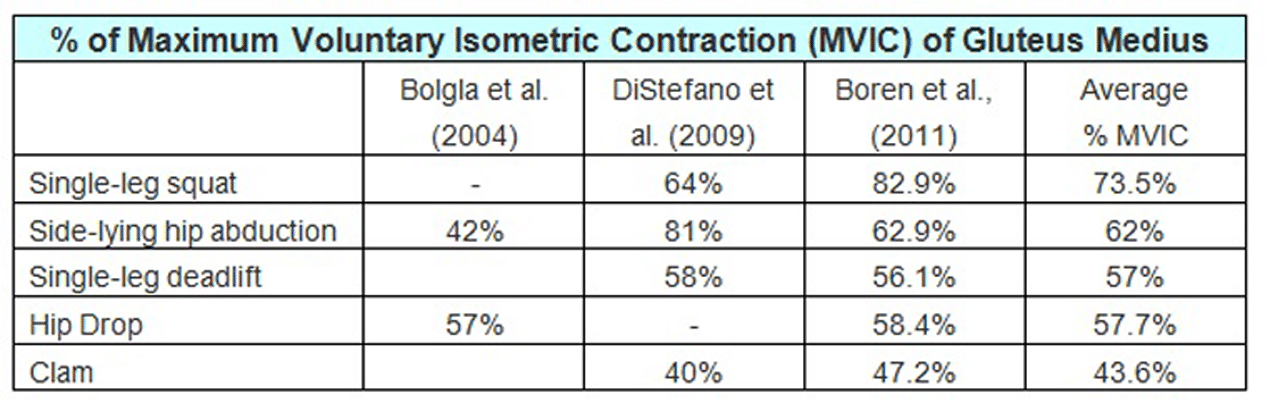
Other studies have been done including research for exercises not included in the three studies above (Ayotte et al.,2007; Krause et al.’2009; Philippon et al., 2011) but none of them weaken the relevance of the data in the table. It is worth pointing out that the variance in results may be due to the technique used in execution of each exercise.
However:
Which exercise/s you do will depend on your individual circumstances, needs and goals, all of which should be considered by a professional before you start a new program.
For example, although single-leg squats score the highest MVIC% in the table, they may not be appropriate for you at this moment in time if you are suffering from a patellar tendonitis.
All exercises can and should be regressed/progressed according to your personal fitness level. As always, if in any doubt, consult a suitably qualified health professional.
You might be wondering:
What are the five exercises listed in the table? We will describe them here, but the number of repetitions, sets, tempo and breathing patterns given serve as examples only, and may need modifying to suit individual needs & goals.
Single-leg squat

There is rarely ever just one way to perform an exercise. The method of execution will often vary according to what you are trying to achieve. In order to maximize use of the Gluteus medius (and indeed the whole of the Glute family), I personally encourage single leg squats that involve moving the centre of gravity backwards as opposed to forwards. In this case:
- The exercise is initiated by moving your backside backwards and downwards, as opposed to moving the knee of your supporting leg forwards. This can be challenging for many people as it requires a certain level of balance, coordination and flexibility.
- For this reason, the single-leg squat is often placed higher up on the ladder of exercise progression. Attempting it too early will often mean you resorting to moving your knee forwards, which in my opinion reduces recruitment of the glute muscles and puts more stress on the quadriceps muscles and knees.
- In order to encourage initiation of the exercise with a backwards shift, I often recommend clients place a suitably heighted chair behind them to give them a target and confidence in the fact that if they do lose stability they will not be falling onto a hard floor.
- If you are moving backwards, the natural position for the non-weight bearing leg will be in front of you as opposed to behind (see photo).
- As your strength and balance improves, you can progress by lowering the height of the object behind you.
- Whilst the edge of your bed may be a good place to start, it may well not be long until you are using the seat of the toilet as your goal.
Number of repetitions: 10-20 each leg
Number of sets: 1 on weaker leg (if applicable), 1 on stronger leg, 1 again on weaker leg.
Tempo: 3 seconds down (breath in), 1 up (breath out), 2 hold (keep breathing out)
Side-lying hip abduction
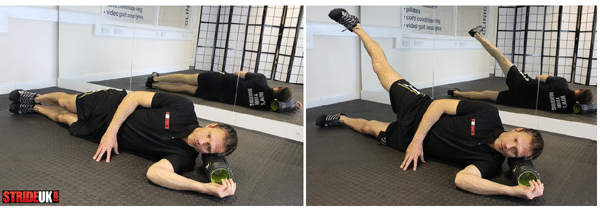
To work the right hip abductor muscles (as in the photo):
- Lie down in a left side-lying position. Make sure your hips are “stacked” (right hip directly over the left hip) and that your body is in a straight line.
- Placing your top hand on the floor in front of you can help ensure that you are not leaning forwards.
- Your pelvis should be in a neutral position (not hitched or tilted forwards/backwards).
- Though performance tempo can vary according to the goal, I typically have a client move accelerate when moving away from gravity, and decelerate when moving in the same direction as gravity.
- In the case of this exercise therefore, I would take 1 second to lift the top leg up (breathing out), 2 seconds to hold it in top position (keep breathing out) and then 3 seconds to slowly return it to start position (slowly breathing in).
- The position of the heel can be varied according to goals, but as a starter I typically encourage the heel to remain the same height as the toes throughout.
Number of repetitions: 15-25 each leg
Number of sets: 1 with weaker side (if applicable), 1 with stronger side, 1 again with weaker side.
Tempo: 1 up (breath out), 2 hold (keep breathing out), 3 down (breath in)
Single-leg deadlift

The single-leg deadlift can be performed in various ways but essentially your aim is to hinge forwards and reach your hands towards the ground whilst keeping your shoulders back, your back straight, and your supporting leg as straight as possible.
- From here you return back up and then repeat. In some versions of this exercise, the non-weight bearing leg is lifted to become as close as parallel to the ground as possible. (I kind of wish I had done this now in the photo – would have looked far more impressive!).
- Progression can involve using weights and/or performing the exercise on a less stable surface. Rotation is also often added to help encourage alignment of the hips.
As well as strengthening the Glutes, single-leg deadlifts can also be an excellent exercise for the hamstrings.
Number of repetitions: 10-20 each leg
Number of sets: 1 on weaker leg (if applicable), 1 on stronger leg, 1 again on weaker leg.
Tempo: 3 seconds down (breath in), 1 up (breath out), 2 hold (keep breathing out)
The hip drop
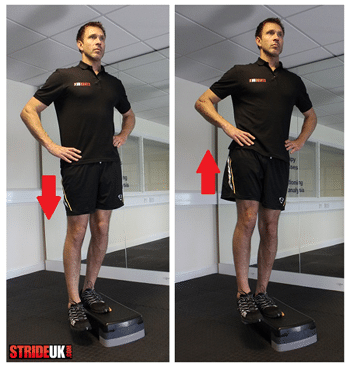
Hip drops, also referred to as pelvic drops, in effect mimic the hip drop we saw can happen during running if the Gluteus medius is not functioning optimally.
- Throughout this exercise, the supporting leg needs to remain straight as all movement needs to be a product of lifting and lowering the hip on the opposite side.
- The body will typically “cheat” on the way down by bending the supporting knee (instead of lowering the opposite hip) and “cheat” on the way up by raising the shoulder (instead of lifting the hip).
- As is the case in all the exercises, try to avoid allowing the pelvis to rotate forwards or backwards.
All exercises typically require quality of movement to achieve goals but this exercise in particular often falls prey to the body finding alternative ways to getting the job done.
Number of repetitions: 15-25 each leg
Number of sets: 1 on weaker leg (if applicable), 1 on stronger leg, 1 again on weaker leg.
Tempo: 2 seconds down (breath in), 2 up (breath out), 2 hold (keep breathing out)
The clam
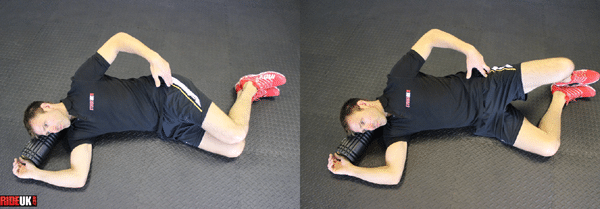
The Clam is typically slandered by advocates of “functional training” but as we have seen research does show they should be considered depending on the needs of the client. I also find them a wonderful way to discover strength imbalances between the two hips.
- In side-lying position, slide your bent legs forward so that your hips are flexed to approximately 30 degrees (other versions of the exercise use different angles).
- Making sure your hips are “stacked” and (apart from your knees) the rest of your body is in a straight line, open your knees while keeping your heels together and pelvis in a neutral position (not hitched or tilted forwards/backwards).
- Placing your hand on the side of the hip should help you feel the Gluteus Medius contracting as the legs open.
Number of repetitions: 15-25 each leg
Number of sets: 1 with weaker side (if applicable), 1 with stronger side, 1 again with weaker side.
Tempo: 1 up (breath out), 2 hold (keep breathing out), 3 down (breath in)
Closing thoughts
I will finish by reiterating that selection of exercise needs to be based on factors, hence the need for therapists & trainers to treat the body in front of them as opposed to what they have read in a book.
As a performer of exercise, it is vital to follow a progressive program and take time to listen to the body. The research we have looked at does serve to remind us, however, that in a world where information is so quickly gained & shared, many exercises being prescribed today do run the risk of being too complicated.
Heres the kicker:
The five exercises we have looked at should not be overlooked because of their age or simplicity. All the evidence suggests that the hip abductors play a very important role in running performance and injury avoidance, so if you need somewhere to start, the lonely Clam may not be such a bad idea!
If you’re interested in learning more about how to improve your own running form and develop the most efficient stride for YOUR biomechanics, signup for our 6-week online form course. The online course will help you run with proper form by teaching you the science of running biomechanics and provide you with a simple-to-follow, progressive set of exercises, drills and mental cues to help you make lasting changes to your form.
RunnersConnect Insider Bonus
Download your FREE Hip Strengthening Exercises Guide inside your Insider Members area.
Download a video and PDF version of the 5 most effective hip exercises for runners. You’ll get more images, full descriptions on how to perform and a video to help guide you.
Not a RunnersConnect Insider member? It’s FREE to join. Click here to get started
Matt Phillips is a Running Injury Specialist & Video Gait Analyst at StrideUK & Studio57clinic. Follow Matt on Twitter: @sportinjurymatt



42 Responses
Great article, very helpful!
Hip strengthening is definitely an area I need to work on.
Time to start doing those exercises…
Hey Chris! Glad you enjoyed it. Thanks for sharing. Always great to hear comments, good or bad!
Thank you for facts as well as exercises. I’m working on my hip strength and the article is a good motivator to keep it up.
Hey Nick. Glad you have found it useful. Thanks for your comment!
How often do you recommend doing these exercises? I’ve been trying to do them everyday – is that too often? Thanks.
Hi Janet. Good question! Tricky to answer!
The frequency, intensity and duration of any exercise will depend on your level of fitness, your individual needs & goals. For any exercise that is new to the body, whatever the level of fitness, it is always wise to introduce yourself carefully and give your body time to let you know how it feels about what you have subjected it to!
In the early days, much of the effort will be concentrating on technique. I find it useful to look at it as follows (although it is a simplification): You are targeting a muscle/muscle group that your body has not used optimally for who knows how long, and your body has found an alternative way of producing the movement using alternative muscles that are now more than ready to step in and get the job done! Unless you watch yourself carefully or have someone watch you, your body will naturally use the alternative methods it is had grown accustomed to using (commonly referred to as “cheating” or “compensating”) until through repeated use the weaker muscles/muscle groups present themselves as a viable alternative.
How long it takes to be able to perform the exercises with good form will depend on the individual. Some people need to do a little everyday, some people every other day. Once you are performing them well and able to concentrate on gradually increasing number of repetitions, advice on how often you perform them will vary from trainer to trainer and will depend a lot on your lifestyle and time available. Ultimately, I am a believer of ensuring your hard training days are hard, and your easy days easy. This helps promote recovery and reduce risk of over-training. With that in mind, I often recommend doing conditioning the same day as your more intensive run, leaving the easy day for relaxing, recovering and listening to your body. But it will depend on the individual!
Hope that helps Janet!
Aloha Matt,
I’ve been running ultras up to 50mi for the past 2 years and I’m having a recurring in jury show up again pes aserine area/ any suggestions on strengthening this area?? I took some time off like a month or so/ I’m able to run again but downhills seam to aggravitite some. I have a 100mi this Sept with 22k of E.G and E.L.
Mahalos for your time
Kade
Great advice. Working in strength training is always a challenge when you’re doing high miles, but so, so important. If you only had 15 minutes a day, what would you recommend?
Hi I have weak right hip, I do single leg deadlift standing on my right and I am about to fall over but if I do it on my left everything is fine!
I also have right hip sometimes popping back in forth on the right hip, is that a sign of a weak hip?
I’m 22 and basketball player, and I PLAY a lot. I recently had some knee pain on my right side as well, could this help?
Hey Skip. Thanks for the question. With regards to your “popping”, can’t diagnose without proper assessment but if it’s accompanied by pain I’m always a fan of getting these things checked out. Given the relatively less stability you experience when standing on right leg does sound like you would benefit from some strengthening exercises. Knee pain is often related to what’s going on in the hip, so could be connected.
Like I say, best to get it checked but in the meantime think about performing hip exercises that involve you moving the hip in ways you do not normally move it (as long as there is no pain). You can download a free Runners Connect hip routine here: https://runnersconnect.net/hip-strengthening-for-runners/
A few weeks of new, run specific strength & mobility training can often make many niggles disappear. Frequently works better than attempting to target a specific muscle. Variety of motion provides the lotion!
Let us know how you get on!
Great article! Do you think this weakness is why one of my feet splay out when I my leg up?
Whenever I see photos or videos of me running, my right foot is always splaying out 🙁
This is very likely. It could also be a glute issue, but closely related.
I develop Piriformis syndrome when I am at the end of training for a long race (for me currently half marathons but I am looking to do a full next year). It is always on the same side (right) and really impedes my pace and frankly my love of being on the road. I work at a desk during the day which means pretty regular pain (isolated and not radiating) when this is acting up. I feel a difference in my gait from left to right which to me means I may have some weakness on the right side that is contributing to my issue. I am very fit and attend boot camp several times a week along with regular running. I am going to try the above exercises. Do you have anything else you would recommend I try?
Thanks for posting the article. I feel like I am finally getting to root of the problem and can hopefully do something to alleviate and get back on the road.
Hi,
Just wanted to say thanks for this post.
I developed some severe knee (and then as a result, hip pain) from long-distance cycling. Had this pain for over a year and couldn’t manage to sort it out. Even resorted to an MRI scan (which didn’t reveal anything interesting).
Following these exercises every other day for 6 weeks has pretty much cleared the pain up entirely (in combination with some hip stretches).
FWIW I could barely even stand on my left leg initially. Now I can do 15 single leg deadlifts with relative ease.
Cheers,
Dan
Hey Dan, really good to hear this helped clear up your knee and hip pain. Doing one’s “homework” is such a crucial part in recovery so it’s great to hear your consistency over 6 weeks paid off. Thanks for sharing!
Thank you so much for this, I have been searching for hours and hours after being diagnosed (via MRI) with Gluteus Medius Tendonitis. Its been 3 months of pain, nothing was helping, tired of spending $ on PT, I am going at this alone with all these exercises! Thanks again <3 this !
I had to hip fracture in January 2013 due to a car accident and went through hip pinning surgery. We are at a year later now. I had to stop PT in May 2013 because insurance wasn’t going to cover more sessions and I was heading back to work. I am 28 year old female. I don’t think I am back at where I need to be, strenght wise. Still have a slight limp. I should have continued PT at home, regret not keeping up with it! I will now be consistent with it! Will these exercises help a year post surgery?
I have been doing hip strengthening regularly while I have been recovering from a metatarsal stress fracture (left foot). Prior to the injury, I had noticed for quite some time it seemed my right knee would bend more than the left during running. I have read through this post several times, and am saw that that greater knee bend is often caused by weak glute medius. Would that indicate the weakness is on my left side (less knee bend), or the right side (greater knee bend)?
Thank you for a very thorough and insightful article. I appreciate your use of references and research to back up your statements. For the single leg squat, can you tell me of any comparison to chair pose from yoga? Is it comparable, or rather, just as good, better or worse?
I have IT band syndrome in my left and it’s really flaring today. I also has SI joint dysfunction, but I find the more I exercise, the better I feel. But it’s too painful right now to get into my T25 exercises or the elliptical.
Thanks.
Hey Michelle,
Many thanks for your feedback! As far as I can see, there are many variations of the single leg chair pose just as there are of a single leg squat, and so there should be! Variety is great, it’s exactly what the body and brain needs. That said, different versions will suit different people with different objectives. With runners, I commonly see over dependence on the anterior muscles of the legs (quads) rather than the posterior (glutes and hamstrings) so I tend to have them do single leg squats / chair pose with the knee behind the toes and weight off the toes. What the non weight bearing leg does will also depend on the needs of the runner. Externally rotating it and tucking it into the weight bearing leg may be a common yoga pose but will my runner benefit from that external rotation? With regards to your ITB Syndrome, I would need to assess you first but I may well have you back off the single leg squats as they could possibly add to the issue. My recommendation would be to see a therapist who specializes in running injuries to assess your ITB issue. Exercise choice can play an important part in rehabilitation and recovery. The fast nature of T25 / Insanity style workouts may need modifying for a short time. Keep in touch!
The problem with a lot of these exercises is that a lot of them are difficult to perform at the beginning and it’s hard to progress them. The lying down exercises are ok in the beginning of rehab but will not restore full functionality. The single leg squat is good but it tires your quads and hamstrings so quickly.
The best exercise i have found is the standing single leg row.
You tie an elastic band onto a door handle, stand half a metre away from the door, balance on one leg and pull the band towards your waist whilst remaining balanced.
You will notice that on your stronger leg you will be able to stand further away from the door and maintain balance. The goal is to gradually increase the weak glute’s strength so that you can move further and further back until it matches the strength of the stronger glute.
I hope this exercise helps, it is one that is easy to progress.
Hi Matt,
Great article!
I’m currently about six weeks into rehabbing a PFPS injury that came on during a marathon training in April. I’m just about ready to start running again (I think) and am wondering if you have any exercises to add to this routine.
Weighted single leg raises have also been a part of my routine but am still avoiding the deep squatting exercises as to not aggravate the knee. Also, would you recommend doing these strength exercises before or after running?
Thanks for any insight…
Bill
Hey Bill, many thanks for your comments – great to hear you are on your way to returning to running!
As far as more exercises for the glute med, there are plenty more than I shared here dependent on what stage you are at.
One important angle to look at is that in running the glute med works on the weight bearing leg, i.e stops the opposite hip from falling too much. In order to recreate this it is useful to include exercises that work the glute med in this way. A favourite of mine is standing say on your left leg with your right leg raised to hip height, (knee bent to 90°) and your bent right leg pushed into a wall or mirror. This position forces your legt glute med to hold the right pelvis up. To make it harder, hold a weight (e.g. a med ball) out infront of you and rotate your upper body over the stabilising left leg. A few of these and you should really feel your left glute med start working! If you can perform over 20 with good form, consider increasing the weight.
For more exercises, consider our Runners Connect Strength Training Package. Many clear & safely progressed exercises there!
Thanks again for your comment! Let us know how your return to running goes. Here’s a link for the Strength Package: https://runnersconnect.net/strength-training-for-runners/
I’m a 51 year old male, good health, active. I have had 3 total hips on my right hip. The first 25 years ago because of the pain. I had child hood legg-calve-perthes (osteochondrosis) causing me pain later in my adult life. The next was 4 years ago and then one 11 months after that to correct a miss aligned cup installation. Not one Dr. has ever explained to me about my limp, Trendelenburg gait. I have in the last couple weeks been reading everyting I can find about it. 2 weeks ago I had a PRP (platelet rich plasma) Intra-articular Injection on my knee of the good leg. I believe my limp is causing my knee problems. And just maybe if I can correct my limp by doing your exercises I bet my knee will also be able to heal. I will start today with them and keep you informed. Your article has been the most informative to me I have seen yet. Thank you
Any suggestion for spinal stenosis. I love to run but the pain is so bad in my left thigh. I’ve started biking and that’s helped but I want to hit the road again.
Does this exercise allow to a hip replacement patient? Thanks
how many days should i do this a week?
Hi Nick, you will find the best results occur if you do them at least 3 times per week, no more than 5 though! Hope this helps!
excellent article! I’ve started with most of these a year and a half ago and am ready to progress to some more challenges, so I am using a functional trainer with an ankle cuff and kicking out to the side with the moving leg positioned behind the stationary leg to pinpoint the medius better. I was wondering if there might be any advantage to doing these side kicks with the moving leg out in front of the stationary leg instead ? would that concentrate more on the Minimus? would that be a more “balanced” way of training the abductors?
Hello, I am sorry but I am not qualified to answer that question for you. You can reach out to Matt Phillips through his twitter @sportinjurymatt if you would like to ask him. Glad you enjoyed the article 🙂
Hey Matt, I have had trouble with my knees and lower back for a year now. When I squat and deadlift, my lower back rounds and my butt tucks under. This is 100% not a technique issue. A personal trainer and saw me in the gym and he said my hip hinge was brilliant, but that when I get past a certain point everything crumbled, back rounds and backside tucks under. I have been told this could be tight hip flexors, coupled with inactive glutes and weak hamstrings. I cannot confirm this for certain but I am performing exercises to combat this problem. What are your thoughts?
Hi Mike! Thanks for the question. It’s obviously tricky to answer without seeing you in person but what I will say is due to anatomical variance, people should not all expect to be able to squat to the same depth. The shape of the femur head and hip socket have a significant determining factor in how much hip flexion you can get. After that point, the only way to get any lower is a backward rotation of the pelvis and the resulting roundening of the back you are referring to. I don’t know if this is what is happening in your case but worth checking.
Limited ankle dorsiflexion is another factor you may want to check out. Does it make any difference if your heels are raised, e.g. up on a weight plate?
You mention tight hip flexors as a possible issue but in my experience lack of flexibility there is not always the issue. Not that much is really needed during a squat.
If as you have said your technique is good and you have developed the coordination required to do deep squats, I’d check out the two points I have suggested.
Hope this helps and thanks again for a great question!
Matt.
Where should I feel the hip drop? I feel it in the hip on my support leg. Is that right?
It would be difficult to feel it yourself, as you will be so used to it, but others can watch you run and look for it, however, if you do feel it, that means it must be pretty prominent. Yes, it would likely be in your support leg. Hopefully the exercises in this post will help you learn how to strengthen it. You may also enjoy this podcast we did, which talked a lot about running gait https://runnersconnect.net/running-interviews/matt-phillips-gait-analysis/
I wasn’t clear. I meant the exercise called the hip drop, not the drop of the hip when I run. Which muscles should feel the exercise? The ones in my planted, stationary leg?
Hi Gale! Yes, correct. You should feel the gluteus medius of the planted leg contracting (shortening) when you raise the opposite side hip and working eccentrically (lengthening under tension) as you slowly lower that side. Placing your hand over the hip & buttock of the planted leg can help you feel this happening.
I hope that helps and thanks for leaving the comment!
I am hoping that these exercises work for me! I broke my hip in a bad car accident three years ago, and I am tired of using my “unbalanced” hips as an excuse to not run. I broke my hip in four places on my left side, including my sacrum. I did not place any weight on that side for only two months, and it through everything off. I will definitely be trying these suggestions to strengthen my hips, especially on my left side!
Hi Anna, thanks for reaching out. Sorry to hear about your accident. We hope you find this helpful, and there is a very good chance you are going to feel much better after they have time to be effective. Best of luck, let us know if we can help with anything else as you recover.
Hi Anna,
Thanks very much for sharing. I am inspired by the determination I hear in your voice and hope the exercises help your return to running! Bear in mind that you may also need to address your running form as well, as you may well have developed compensatory ways of moving since your accident. A full body gait analysis would be useful to identify any drills you may need to get those hips working well again once you have strengthened them! Thanks again for sharing and let us know how you get on!
203009 8192I conceive this internet web site has got some really superb information for everybody : D. 423289
Matt
Thank you for this article it is just what I need!
I have literally spent the last 16 years trying to work out what the pain in my right glutes and hip area is all about.
Interestingly I have noticed that it is usually runners websites seem to make most sense for me.
Thinking about it at school and in the army in the 80s and 90s I was primarily A cross country runner. I Richard my ACL left side in 1990 and had it reconstructed in 92. 16 years ago I started to get discomfort in my glutes on the right side. Massage and stretching and hot water bottles help, but the problem always comes back especially in the early hours of the morning and prevent me from getting proper sleep.
A Specialist physiotherapist has recently suggested that I probably have a chronic piraformis problem. I think it is only part of the problem however as stretching muscles such as TFL, psoas,hamstrings and IT band really do seem to help.
Anyway to come to the point, I came cross your article searching for hip abductor and adductor exercises. Just ran through the routine once in my lounge and really seemed to exercise just the right muscles and stretch the right muscles too.
Many many thanks and any advice from you would be very gratefully accepted thank you!
Andrew Lewis, Andover, Hampshire.
Sorry, typo, Richard should have been ruptured.