

Your doctor says your blood work looks fine.
Your ferritin is 18 ng/mL, which falls inside the standard reference range of 12 to 300 ng/mL for women.
So you keep training, keep feeling sluggish, and keep wondering why your race times won’t budge.
The problem is that “normal” ferritin ranges were built for the general population, not for people who run 30 to 50 miles a week and destroy red blood cells with every footstrike.
A study tracking 165 female rowers found that 30% had low ferritin with completely normal hemoglobin, and those with depleted iron trained roughly 10 fewer minutes per day and had measurably lower VO2 peak values.
They weren’t anemic or flagged on any standard panel.
They were just slower than they should have been.
So, in this article you’re going to learn the research-backed practical advice on optimal ferritin levels for runners:
- Why the standard “normal” range hides a performance problem most doctors won’t catch
- The 3 stages of iron deficiency and how to tell which one you’re in
- The ferritin targets that research supports for male and female runners
- How training actively drains your iron stores through 5 different mechanisms
- Why a single ferritin test can mislead you and what to order instead
- The supplement forms, doses, and timing strategies that actually raise your levels
Why Does “Normal” Ferritin Leave Runners Underperforming?
Standard lab reference ranges define “normal” ferritin as 12 to 300 ng/mL for women and 12 to 400 ng/mL for men.
Those ranges exist to screen for clinical disease, not to optimize athletic performance.
A meta-analysis of 17 studies found that iron treatment in non-anemic athletes produced moderate improvements in VO2max, confirming that correcting low ferritin improves aerobic capacity even when hemoglobin looks normal.
A runner with ferritin of 15 ng/mL passes every standard blood panel.
That same runner may be losing training quality every single day because iron-dependent enzymes in the mitochondria can’t produce aerobic energy efficiently.
Hemoglobin, the number most doctors focus on, tells you whether your blood can carry oxygen right now.
Ferritin tells you how much iron your body has in reserve to keep making hemoglobin, fueling mitochondrial enzymes, and supporting the hundreds of iron-dependent processes that keep your aerobic system running.
When ferritin drops below 30 ng/mL, your reserves are shrinking even if your hemoglobin looks perfect.
The gap between “clinically normal” and “athletically optimal” is where most runners lose performance they never knew they had.
What Are the Three Stages of Iron Deficiency in Runners?
Iron depletion doesn’t happen overnight, and it doesn’t always show up on standard blood work until the damage is significant.
A 2025 systematic review of 669 female athletes found that iron deficiency reduced endurance performance by 3 to 4% compared to iron-sufficient athletes.
The prevalence of iron deficiency in runners ranges from 15 to 35% in women and 5 to 11% in men.
Iron status progresses through 3 distinct stages, each with different lab markers and different consequences.
- Stage 1: Depleted Iron Stores (ferritin below 30 ng/mL, hemoglobin normal). Your body’s iron savings account is draining, but the checking account still works. No obvious symptoms yet, though training adaptation may already be blunted. This is where most runners sit without knowing it.
- Stage 2: Iron Deficiency Without Anemia, or IDNA (ferritin below 20 ng/mL, hemoglobin normal). Reserves are critically low. Fatigue creeps in, workouts feel harder than they should, and recovery takes longer. Your doctor still says you’re fine because hemoglobin hasn’t dropped.
- Stage 3: Iron Deficiency Anemia, or IDA (ferritin below 12 ng/mL, hemoglobin below normal). Both stores and oxygen-carrying capacity are compromised. Performance drops sharply, and the diagnosis is finally obvious on a standard blood panel.
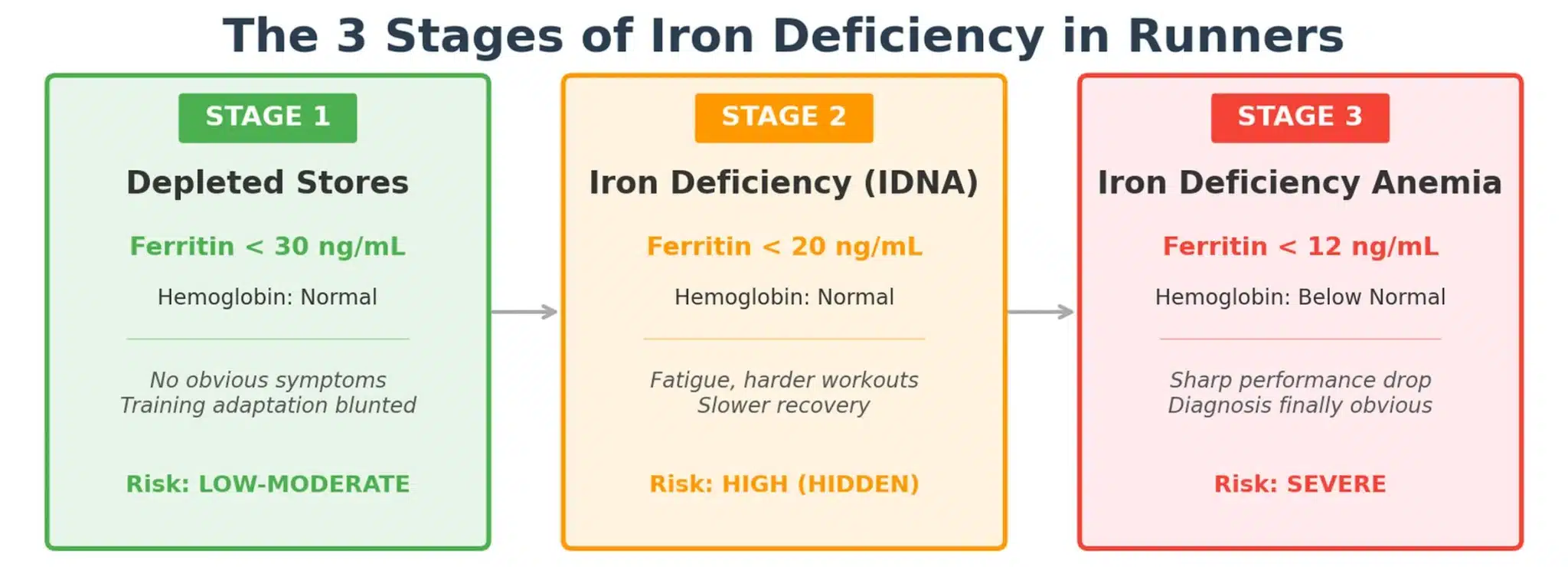
Stage 2 is the most dangerous for runners because it causes real performance loss while producing normal-looking lab results.
A 2004 study demonstrated that iron deficiency without anemia impairs the body’s ability to adapt to endurance training, even when hemoglobin remains in the normal range.
The women in that study who received 100 mg of supplemental iron improved their endurance capacity after training, while those on placebo did not, despite identical training programs.
What Ferritin Level Do Runners Actually Need?
The research points to thresholds well above what standard lab work considers adequate.
A 2023 systematic review recommended athletes maintain ferritin between 40 and 90 ng/mL, with levels above 40 ng/mL needed before altitude training to support increased red blood cell production.
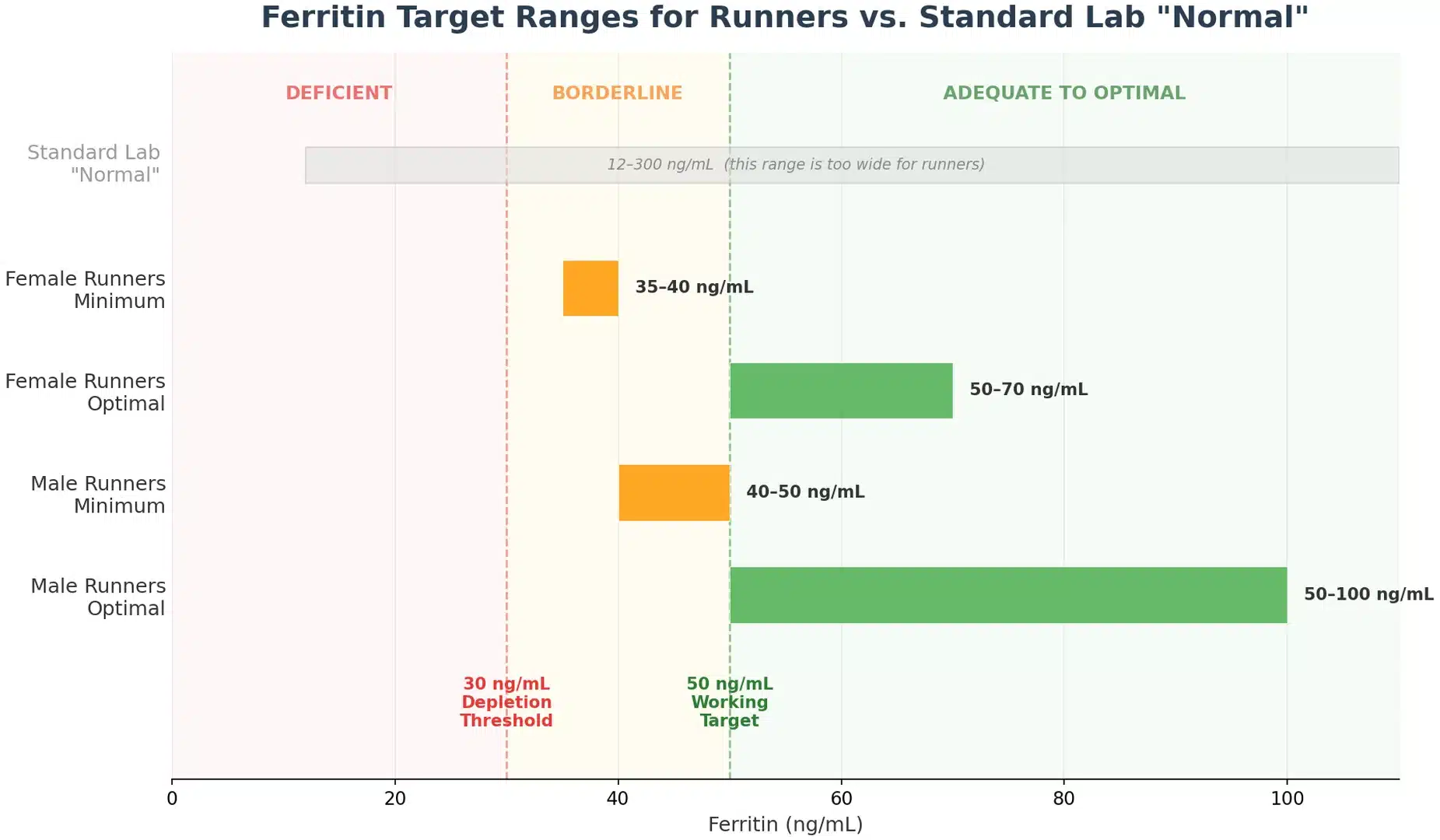
Here’s what the current evidence supports for target ranges:
For female runners:
- Minimum: 35 to 40 ng/mL
- Optimal: 50 to 70 ng/mL
For male runners:
- Minimum: 40 to 50 ng/mL
- Optimal: 50 to 100 ng/mL
These numbers account for a critical factor most target ranges ignore: day-to-day variability.
Ferritin fluctuates by 15% in men and up to 27% in women from one blood draw to the next.
A runner sitting at 30 ng/mL could test anywhere from 22 to 38 ng/mL depending on the day, time, and how recently they did a hard workout.
Targeting 30 ng/mL as a floor means normal fluctuations regularly drop you into deficiency territory during hard training blocks or illness.
Aim for 50 ng/mL as your working target, and you build a buffer that absorbs the natural swings without dipping below the performance threshold.
Why Does Training Actively Drain Your Iron Stores?
Running doesn’t just use iron faster than sedentary life, it actively blocks your ability to replace what it takes.
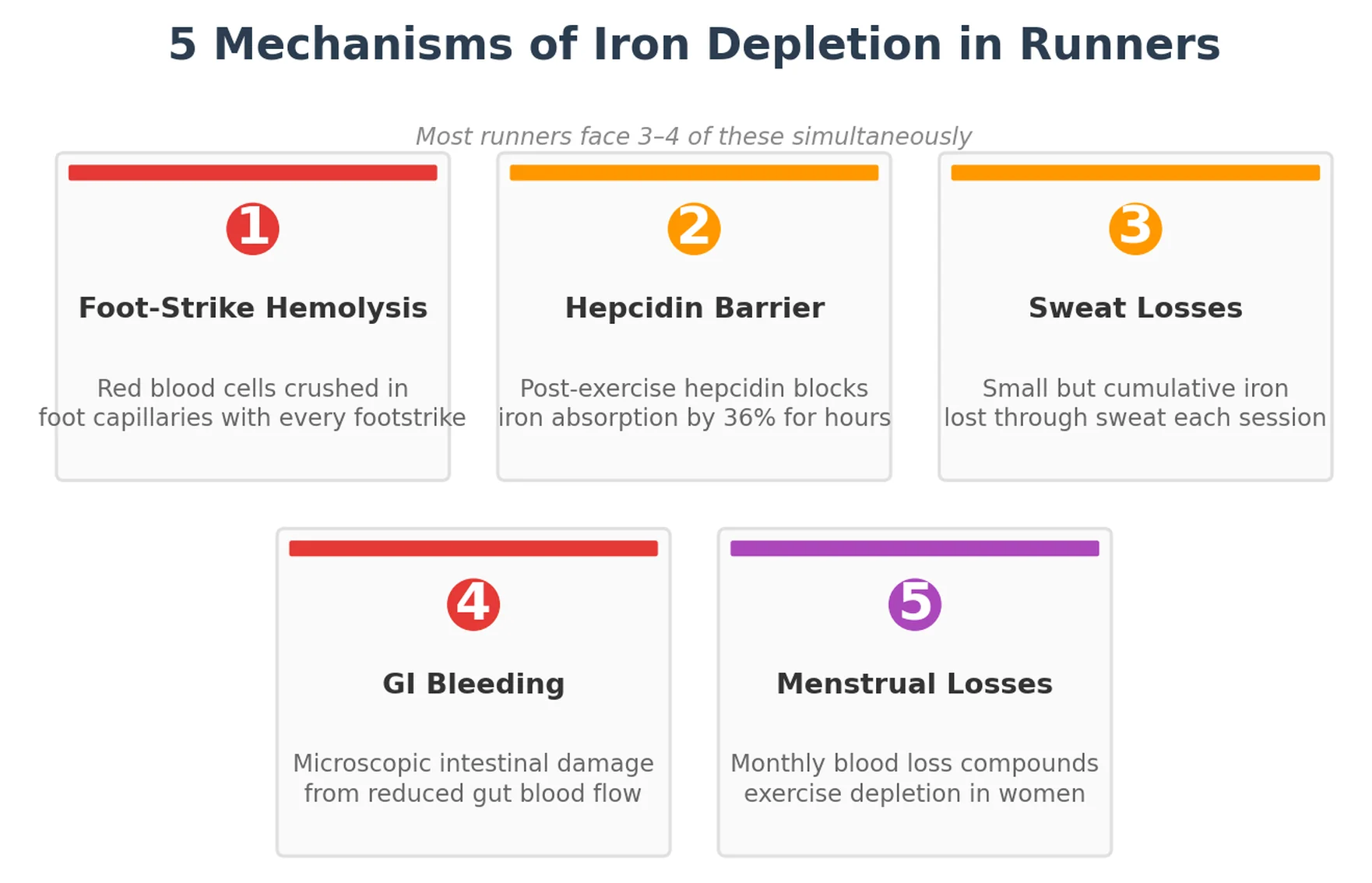
Your body loses iron through at least 5 separate mechanisms during training, and 1 of them directly sabotages the absorption of iron you eat or supplement after workouts.
Does Running Destroy Red Blood Cells?
Every footstrike crushes red blood cells in the capillaries of your feet.
A 2024 scoping review of 267 runners found that haptoglobin, the protein that cleans up damaged red blood cells, dropped 21% after long-distance races, while reticulocytes (new replacement cells) increased 16%.
This process, called foot-strike hemolysis, happens on every single run.
The iron released from destroyed red blood cells gets recycled, but the process is imperfect, and daily or twice-daily hemolytic episodes during hard training blocks create a cumulative drain.
How Does Hepcidin Block Iron Absorption After Training?
Hepcidin is a hormone that controls how much iron your gut absorbs and how much stored iron your body can access.
A study of 28 trained cross-country runners found that hepcidin increased 51% after a prolonged run, and fractional iron absorption dropped 36% compared to resting conditions.
The spike happens because running triggers interleukin-6, an inflammatory signal that ramps up hepcidin production 3 to 6 hours post-workout.
The iron-rich meal you eat right after a long run faces an actively hostile absorption environment in your gut.
Your body absorbs 36% less iron in the hours after a hard run than it would at rest.
Research on elite rowers during a 4-week training camp showed hepcidin doubled from baseline within the first week of intensified training, confirming that high training loads sustain elevated hepcidin well beyond a single session.
What Other Mechanisms Deplete Iron in Runners?
Sweat losses.
Iron is lost through sweat during every training session. The amount per session is small, but it compounds across months of consistent training, especially in hot conditions.
GI bleeding.
Reduced blood flow to the gut during running causes microscopic intestinal damage that leads to small but chronic iron losses through the GI tract.
Menstrual losses.
A 2025 study of female athletes found a significant inverse relationship between menstrual blood loss and ferritin levels. Female runners face a compounding challenge: menstrual losses plus exercise-induced depletion plus hepcidin-mediated absorption barriers create a triple drain that male runners don’t experience.
Does Low Ferritin Affect More Than Your Endurance?
Iron plays a direct role in producing dopamine, serotonin, and other neurotransmitters that regulate focus, motivation, and decision-making.
Research on iron status and cognitive function found that both very low and very high ferritin levels impair cognitive performance, creating a U-shaped relationship where the middle range produces the best outcomes.
Participants who improved their ferritin levels showed measurable gains in attention and impulse control compared to those whose levels stayed flat.
For runners, this means that the mental fog, poor pacing decisions, and inability to push through discomfort in the final miles of a race may not be a willpower problem.
Low iron directly compromises the brain’s ability to regulate effort and sustain focus under fatigue.
The same symptoms, persistent tiredness, declining motivation, difficulty concentrating, also overlap almost perfectly with overtraining syndrome. The signs of iron deficiency and overtraining present identically, and blood testing is the only reliable way to distinguish them.
Rest alone won’t fix an iron deficit.
Why Can’t You Trust a Single Ferritin Test?
Ferritin is an acute-phase reactant, which means your body produces more of it whenever inflammation is present, regardless of how much iron you actually have stored.
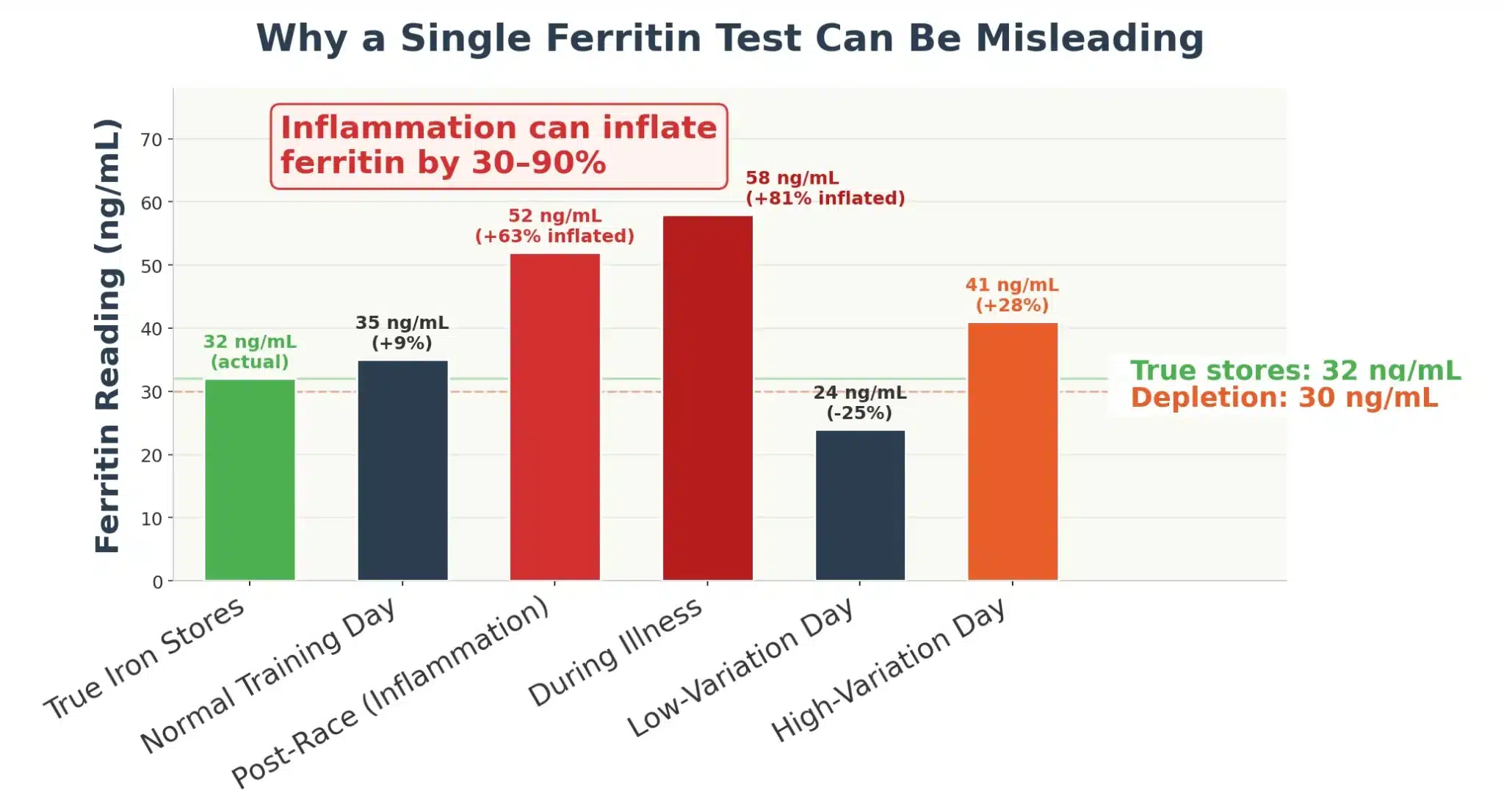
Studies have shown that inflammation can inflate ferritin readings by 30 to 90%, masking true iron deficiency behind a number that looks adequate.
A hard race weekend, a lingering cold, or even intense psychological stress can transiently lift ferritin through inflammatory signaling rather than actual iron storage.
A runner who tests ferritin at 50 ng/mL the Monday after a marathon may actually have functional iron stores closer to 25 to 35 ng/mL once the inflammatory spike resolves.
Day-to-day variability adds another layer of uncertainty.
Ferritin swings by 15% in men and 27% in women under normal conditions, with individual athletes showing swings as wide as 44%.
A single ferritin number without context is a snapshot, not a diagnosis.
C-reactive protein, or CRP, is the key to reading ferritin accurately.
High ferritin combined with high CRP means inflammation is driving the number up, and true iron stores may be much lower than the test suggests.
High ferritin combined with low CRP means the reading reflects genuine iron storage.
Soluble transferrin receptor, or sTfR, provides a second confirmatory marker. sTfR rises when your cells are genuinely hungry for iron, and it isn’t affected by inflammation.
How Should Runners Test and Interpret Their Iron Status?
Testing ferritin alone is like checking only your oil light and assuming the whole engine is fine.
Request this panel from your doctor:
- Serum ferritin to measure iron stores
- Complete blood count (CBC) to assess hemoglobin and red blood cell indices
- C-reactive protein (CRP) to check for inflammation that may inflate your ferritin reading
- Serum iron and transferrin saturation for a fuller picture of iron availability
- Soluble transferrin receptor (sTfR) if ferritin and CRP results are ambiguous
When to test:
Test during a normal training week, not after a race or unusually hard block. Avoid testing within 72 hours of a hard effort, since both inflammation and hemolysis can distort your results.
How to interpret your results:
Ferritin below 30 ng/mL with normal CRP: true iron depletion. Start oral supplementation at 25 to 100 mg elemental iron daily, optimize dietary iron, and retest in 8 weeks.
Ferritin 30 to 40 ng/mL: borderline for athletes. Maintain aggressive dietary focus, consider low-dose supplementation during high-volume training blocks, and monitor closely.
Ferritin above 40 ng/mL with normal CRP: adequate stores. Maintain through diet, test periodically (every 3 to 6 months during heavy training), and supplement only if levels decline.
Ferritin appears normal but CRP is elevated: your true iron status may be lower than the number suggests. Wait 2 weeks for inflammation to resolve and retest, or request sTfR as a confirmatory marker.
What’s the Most Effective Way to Supplement Iron?
The form of iron you take matters as much as the dose.
Standard over-the-counter iron supplements use ferrous sulfate, the cheapest and most common form.
Your body absorbs only 10 to 15% of iron from ferrous sulfate, leaving 85 to 90% sitting in your digestive tract where it causes nausea, constipation, and cramping.
Those side effects are the primary reason runners stop taking iron supplements before they see results.
A randomized trial found that 25 mg of iron bisglycinate was non-inferior to 50 mg of ferrous sulfate for preventing iron deficiency, with significantly fewer gastrointestinal complaints.
Iron bisglycinate is a chelated form where glycine molecules protect the iron through stomach acid and deliver it to the small intestine for absorption.
The result is better uptake at a lower dose with fewer side effects, which means you actually keep taking it long enough for the levels to move.
If you’re looking for an iron supplement made specifically for runners, I highly recommend checking out MAS Iron.
Their formula combines iron bisglycinate with other cutting-edge ingredients like Alpha GPC that are specifically designed for endurance athletes who need to increase iron levels without the stomach issues that come with standard supplements.
When Should You Take Iron Relative to Training?
Hepcidin, the hormone that blocks iron absorption, follows a diurnal rhythm. Levels are lowest in the early morning and rise throughout the day.
Training pushes hepcidin even higher, peaking 3 to 6 hours post-exercise.
Take iron first thing in the morning on an empty stomach, or at least 6 hours after your last hard workout.
If you train in the morning, take iron in the evening, at least 6 hours post-session.
That said, research on dancers with sub-optimal iron found that morning vs. evening supplementation produced equivalent results over 8 weeks.
Consistency matters more than perfect timing.
What Dietary Strategies Support Iron Absorption?
Pair iron-rich foods with vitamin C at the same meal. Vitamin C dramatically improves non-heme iron uptake even in the presence of absorption inhibitors like phytates and polyphenols.
Avoid taking iron with calcium, coffee, or tea, all of which reduce absorption.
For plant-based runners, iron bioavailability from non-heme sources ranges from 1 to 5% compared to 10 to 20% from heme iron in animal products. But maximizing iron absorption through strategic food pairing and vitamin C can close much of that gap.
Whether you need an iron supplement depends on your current ferritin level, your diet, and how much iron you’re losing through training. Testing gives you the answer.
When Should Runners Consider IV Iron?
Oral supplementation works for most runners, but some can’t tolerate it or don’t respond quickly enough.
Research on distance runners showed that IV iron rapidly increases ferritin stores within 6 weeks and improved training set times at the 2-week mark.
A separate study found that 4 weeks of IV iron reduced perceived fatigue and mood disturbance in trained athletes, even those without a clinical iron deficiency diagnosis.
IV iron is a medical intervention, not a performance shortcut.
It’s appropriate when oral supplementation causes intolerable GI side effects, when ferritin remains critically low after 8 to 12 weeks of consistent oral supplementation, or when rapid restoration is needed before a key competition or altitude training camp.
Discuss the option with a sports medicine physician who understands athletic iron needs.
| Iron Factor | What Happens | What to Do |
|---|---|---|
| “Normal” lab ranges | Ferritin of 12-30 ng/mL passes standard screening but leaves athletes underperforming | Request athlete-specific interpretation; target 50+ ng/mL |
| Foot-strike hemolysis | Red blood cells destroyed with every footstrike; haptoglobin drops 21% after long races | Account for cumulative losses; test regularly during high-mileage blocks |
| Hepcidin post-exercise | Iron absorption drops 36% for several hours after hard training | Take iron supplements 6+ hours after training or first thing in the morning |
| Inflammation masking | CRP elevation inflates ferritin 30-90%, hiding true deficiency | Always test CRP alongside ferritin; retest 2 weeks after illness or hard race |
| Menstrual losses (female runners) | Monthly blood loss compounds exercise-induced depletion | Test more frequently; consider higher ferritin targets (50-70 ng/mL) |
| Supplement form | Ferrous sulfate: 10-15% absorbed; 85-90% causes GI distress | Use iron bisglycinate for better absorption and fewer side effects |
Ferritin measures the iron reserves your body draws on to make hemoglobin, fuel mitochondrial enzymes, and sustain aerobic performance.
Between 15 and 35% of female runners and 5 to 11% of male runners are iron-deficient, often without knowing it, because standard lab ranges define “normal” as low as 12 ng/mL.
Running drains iron through foot-strike hemolysis, GI blood loss, sweat, and menstrual losses in women.
Training also raises hepcidin, a hormone that reduces iron absorption by 36% in the hours after hard exercise.
Ferritin levels fluctuate by 15 to 27% day to day, and inflammation can inflate readings by 30 to 90%, making a single test unreliable without a concurrent CRP check.
Research supports a minimum ferritin target of 35 to 40 ng/mL for female runners and 40 to 50 ng/mL for male runners, with optimal performance at 50+ ng/mL.
Iron bisglycinate supplements absorb better and cause fewer GI side effects than ferrous sulfate, the most common pharmacy form.
Testing serum ferritin alongside CRP, CBC, and sTfR gives the most accurate picture of your true iron status.



