

If you’re a female runner who’s ever dealt with knee pain, you’ve likely heard an explanation: female runners are more susceptible to knee pain than male runners because they have wider hips.
You might have come across the term Q Angle, and been told that because your angle is greater, your knees are under more strain. Maybe you’ve been told your knees are misaligned or “maltracking” (moving wrong).
It’s true that men and women have anatomical differences in hip and leg structure.
It makes sense that these differences could affect running form subtly.
But here’s the critical question: do these anatomical differences actually cause knee pain?
The research says no. And that changes everything about how you should approach prevention and recovery.
So, in this article you’re going to learn the research-backed practical advice on:
- What patellofemoral pain (runner’s knee) is and how it’s diagnosed
- Why the Q angle explanation is incomplete and sometimes wrong
- The real reason female runners get more knee pain (spoiler: it’s not your anatomy)
- How pain thresholds work and why progressive loading beats rest alone
- The framework for actually recovering from runner’s knee
The Q angle (quadriceps angle) is the angle at your kneecap between your thigh line and your shin line. Women average 15–20° and men average 10–15°, but research shows Q angle does not predict or cause runner’s knee.
What Is Patellofemoral Pain Syndrome?
Patellofemoral pain syndrome (PFPS), commonly known as runner’s knee, is pain around or beneath the kneecap.
This is one of the most common running injuries, and female runners experience it more often than male runners.
Distinguish PFPS from IT Band Syndrome early: PFPS causes pain on the kneecap’s edges or underneath it, while IT Band Syndrome causes pain on the outside of the knee joint, away from the kneecap itself.
Because treatments differ between these two injuries, getting a clear diagnosis from a professional is essential.
For more on IT Band Syndrome, read IT Band Syndrome in Runners.
What Is Q Angle and How Is It Measured?
The Q angle (quadriceps angle) is measured by drawing a line from the top of your hip (the anterior superior iliac spine) to your kneecap, then comparing it to a vertical line down through your shin. The further your kneecap deviates inward from that vertical, the larger the angle.
Women typically measure 15–20° and men 10–15°, because women’s wider hips create a steeper inward pull toward the knee.
The “Q” stands for Quadriceps, the muscles that run along the front of your thigh.
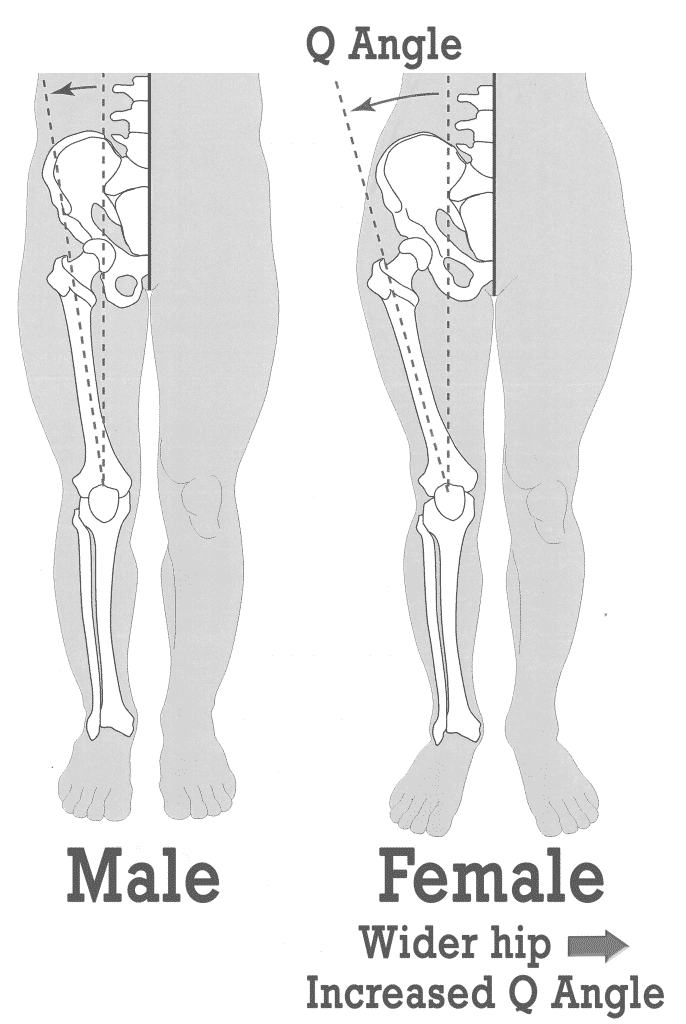
The common belief is that a greater Q Angle puts more strain on your knees. The reasoning goes: a larger angle pulls your kneecap away from its natural groove, creating more friction and pain.
This patella maltracking is thought to cause friction that results in pain around the kneecap, sometimes diagnosed as Patellofemoral Tracking Syndrome (PFTS).
The standard treatment focuses on restoring “normal” knee tracking by strengthening and stretching targeted muscles.
Does Patella Maltracking Actually Cause Knee Pain?
Despite how logical the maltracking explanation seems, the assumption that abnormal kneecap movement causes pain doesn’t hold up under scrutiny. In fact, research on runner’s knee shows something surprising about kneecap mechanics.
The problem is a flawed assumption: humans aren’t built to move in just one “right” way, and any deviation from an arbitrary norm doesn’t automatically cause pain.
Consider two scenarios that challenge this assumption: runners with maltracking knees who experience no pain, and runners with perfectly normal tracking who are in pain.
Research has shown that among runners with and without patellofemoral pain, patellar movement patterns were inconsistent and highly individual, with no single pattern distinguished those in pain from those pain-free.
In a landmark study by MacIntyre et al. (2006), researchers used advanced MRI imaging to track kneecap movement across 60 volunteers in three groups: those with PFPS and visible malalignment, those with PFPS but normal alignment, and pain-free controls.
Results showed no differences in overall patellar motion patterns across the groups. Kneecap spin and tilt varied widely within each group, with nothing unique to the pain group.
The only measurable difference: at 19 degrees of knee flexion, the pain group’s kneecaps sat 2.25 millimeters more toward the outer side than the control group.
Here’s the problem: therapists cannot visually detect a 2.25 millimeter displacement, meaning they can’t identify maltracking by examining a patient, let alone measure whether fixing it will resolve pain.
The study’s conclusion was clear: “An individual with patellofemoral pain syndrome cannot be distinguished from a control subject by examining patterns of spin, tilt, or lateral translation of the patella.”
This finding fundamentally challenges the entire “correct the tracking” treatment model that dominates many physical therapy clinics.
Does Strengthening Your VMO Fix Runner’s Knee?
The Vastus Medialis Obliquus (VMO) is a small muscle on the inside of your thigh. Physical therapists often prescribe VMO strengthening exercises to female runners with PFPS.
The logic seems intuitive: if your knee is being pulled outward by your wide hips and large Q Angle, strengthening the inward-pulling muscle should help rebalance your knee.
It’s an attractive solution: simple, specific, and intuitive. But research tells a different story.
Dissection studies examining cadaverous tissue find no link between VMO size, length, angle, or strength and patellofemoral pain, meaning weak VMOs don’t cause PFPS, and strengthening them doesn’t fix it.
This doesn’t mean VMO work has no place in training.
But it means the rationale for why it should help with PFPS is unfounded. You might spend months on isolation exercises that don’t address your actual problem.
The same applies to other “corrective” approaches: knee bracing, IT Band stretching, and even surgery to “correct” tracking have limited evidence for resolving PFPS.
Why Do Female Runners Get More Knee Pain?
The research confirms one thing: female runners do suffer from PFPS more often than male runners. But the cause isn’t wider hips or a larger Q Angle.
In fact, plenty of female runners have wide hips and maltracking knees yet experience no pain.
Plenty of male runners have normal anatomy but develop PFPS.
This alone tells you that anatomy isn’t the primary driver.
So what is?
Honestly, we don’t know yet. Emerging research is exploring gender-specific injury risk, but conclusive answers haven’t emerged.
What we do know is this: there’s an industry of “biomechanics experts” trained to find structural flaws and sell corrective interventions. Many female runners are funneled into months of “corrective” therapy based on the idea that their bodies are wrong and need fixing.
The biggest risk isn’t your anatomy. It’s spending time and money fixing perceived biomechanical flaws when the real lever for recovery is understanding pain science and progressive loading.
This doesn’t mean biomechanics is irrelevant. Structure matters.
But when it comes to running injury, everything we know points to checking the basics first: training load, recovery, and pain thresholds.
Not anatomical “issues” like maltracking, leg length differences, high arches, or overpronation. These issues often have no link to pain at all.
Understanding Pain, Injury, and Tissue Thresholds
Every tissue in your body has a threshold: a maximum load it can handle before damage results.
When you ask a tissue to do more than it’s capable of, pain signals the warning.
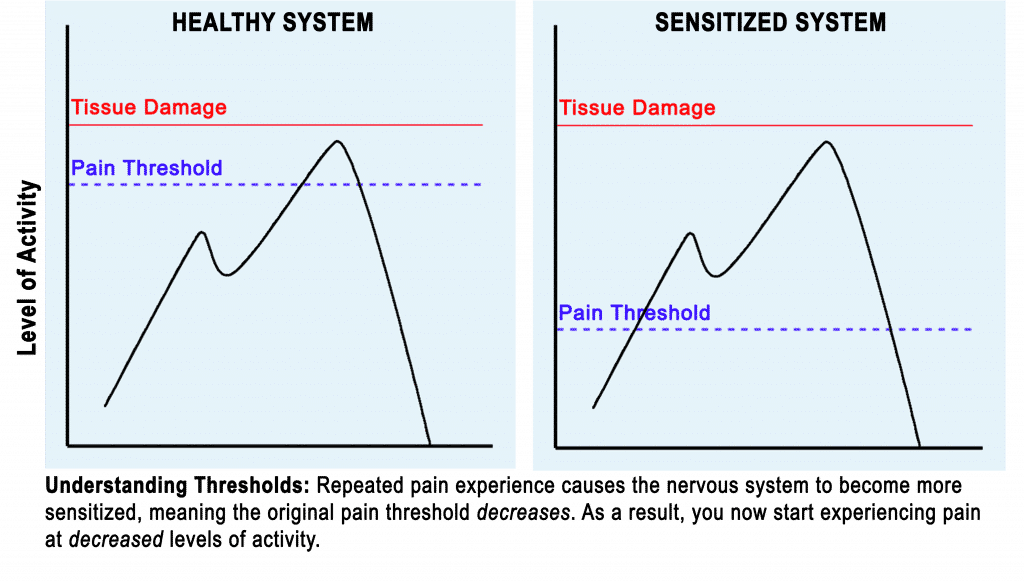
Research has shown that your nervous system has a sophisticated warning system: slightly below the tissue damage threshold sits your pain threshold, where your nervous system signals pain to make you modify your activity.
Pain isn’t your enemy. It’s a protective signal, your body’s defense system.
But here’s where it gets tricky.
After you approach or cross your damage threshold, your nervous system reduces your pain threshold as additional protection.
This means pain starts at a lower activity level than before, giving your tissue time to heal.
If you ignore pain signals and keep pushing, your nervous system protects you further: it reduces your pain threshold even more.
Your system becomes sensitized. Soon, activities that used to be pain-free become painful.
This is why knee pain can progressively worsen, not because your knee is more damaged, but because your nervous system has become increasingly protective.
How Pain Thresholds Change: A Real Example
Picture this: one week you run too much, too fast, or too many days in a row.
During one run, your knee starts hurting at mile 6. You’ve crossed your pain threshold.
You push through or don’t notice. Your body registers tissue threat.
Now you’ve crossed the damage threshold too.
Your body goes into protection mode. The next day, pain starts at mile 4.
A few days later, mile 2. Within a week, walking down stairs triggers pain.
Each time you exceed your nervous system’s current threshold, it lowers the pain threshold further. Your system becomes progressively more sensitized.
This cycle continues until you stop pushing past the threshold, meaning everyday activities that trigger pain must be reduced, not pushed through.
Common activities that quietly exceed thresholds and worsen knee pain include:
- Holding a squat position (at work, gardening, playing with kids)
- Sitting with knees in one position for long periods (desk, car, train)
- Going up and down stairs
- Walking longer distances than your current capacity allows
Why Rest Alone Isn’t Enough for Knee Pain Recovery
In the early stages of PFPS or when pain is severe, rest and system desensitization are crucial. Your nervous system needs time to calm down.
But complete rest is a trap. Your pain thresholds won’t automatically return to their prior levels just because you’ve stopped running.
Recovery requires progressive loading: gradually increasing activity in a way that challenges your tissue just enough to rebuild its capacity without triggering sensitization.
This is where true rehabilitation comes in: not isolation exercises designed to “fix” your alignment, but graded loading guided by a therapist who understands pain science.
The challenge is calibration: too much and you lower your pain thresholds again. Too little and you stay stuck.
Getting this right requires patience and often weeks of careful progression.
Most runners spend 9 out of 10 of these weeks frustrated because progress feels impossibly slow. But this slow, graded approach is what actually works.
How to Return to Running After Knee Pain
Returning to running isn’t about waiting until pain disappears. It’s about starting when pain is manageable and progressing gradually within your current pain thresholds.
Start where you are. Run only as far or as fast as you can without triggering pain.
This is your baseline.
If you can run 2 miles pain-free, start there, not at your old 8-mile distance.
Progress slowly. Add 10% to your weekly volume each week, not distance per run.
If you can run 8 miles per week, aim for 8.8 the following week. Skip a week if pain increases.
Add strength work alongside running. Progressive loading applies to every tissue, not just running-specific ones. 2–3 times per week of basic strength work (squats, step-ups, single-leg balance) helps recalibrate your system.
Know your limits. Pain during running is information.
0–3 out of 10 pain is acceptable. Pain above that signals you’ve exceeded your threshold and need to reduce volume or intensity.
Recovery isn’t linear: consistency over weeks and months beats the temptation of faster progress.



